

Relative contribution of low-density and asymptomatic infections to Plasmodium vivax transmission in the Amazon: pooled analysis of individual participant data from population-based cross-sectional surveys
- PMID: 35663000
- PMCID: PMC9161731
- DOI: 10.1016/j.lana.2021.100169
Relative contribution of low-density and asymptomatic infections to Plasmodium vivax transmission in the Amazon: pooled analysis of individual participant data from population-based cross-sectional surveys
Abstract
Background: Low-density and asymptomatic Plasmodium vivax infections remain largely undetected and untreated and may contribute significantly to malaria transmission in the Amazon.
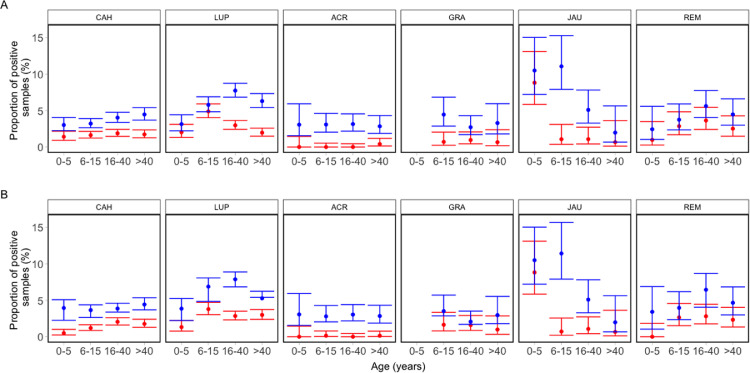
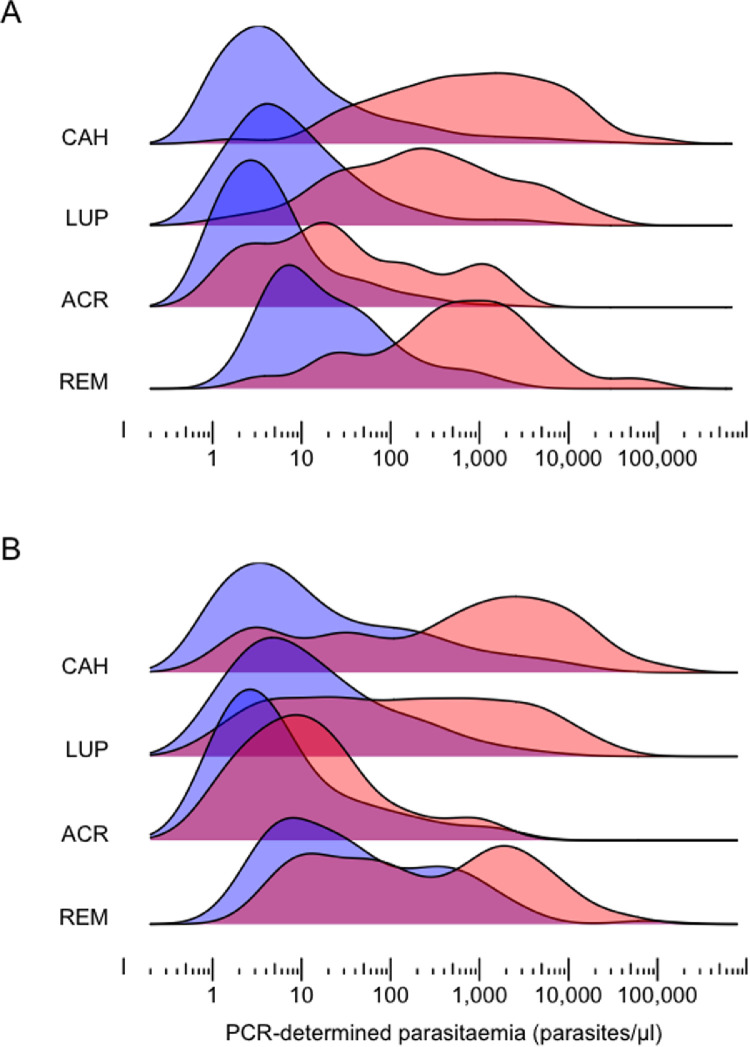
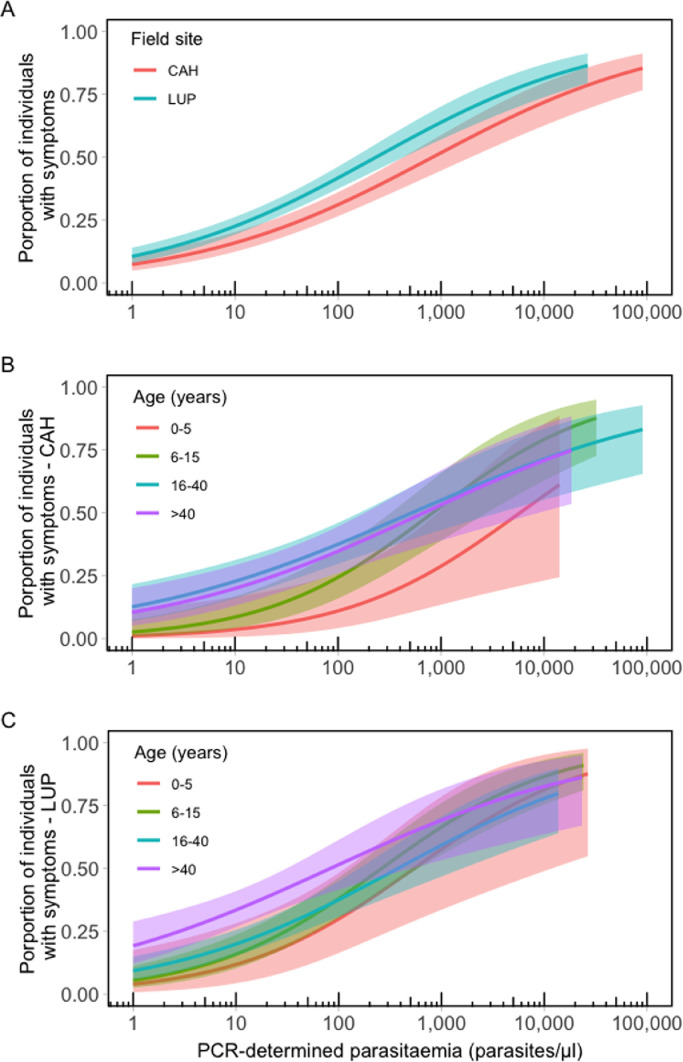
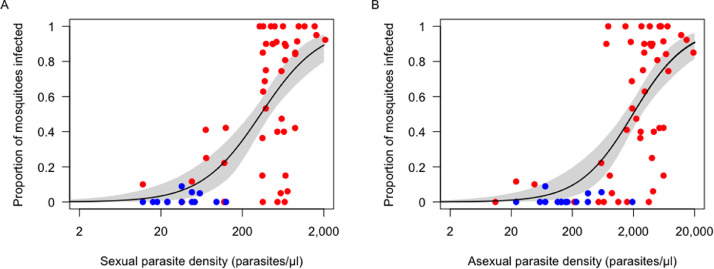
Methods: We analysed individual participant data from population-based surveys that measured P vivax prevalence by microscopy and polymerase chain reaction (PCR) between 2002 and 2015 and modelled the relationship between parasite density and infectiousness to vectors using membrane feeding assay data. We estimated the proportion of sub-patent (i.e., missed by microscopy) and asymptomatic P vivax infections and examined how parasite density relates to clinical manifestations and mosquito infection in Amazonian settings.
Findings: We pooled 24,986 observations from six sites in Brazil and Peru. P vivax was detected in 6·8% and 2·1% of them by PCR and microscopy, respectively. 58·5% to 92·6% of P vivax infections were asymptomatic and 61·2% to 96·3% were sub-patent across study sites. P vivax density thresholds associated with clinical symptoms were one order of magnitude higher in children than in adults. We estimate that sub-patent parasite carriers are minimally infectious and contribute 12·7% to 24·9% of the community-wide P vivax transmission, while asymptomatic carriers are the source of 28·2% to 79·2% of mosquito infections.
Interpretation: Asymptomatic P vivax carriers constitute a vast infectious reservoir that, if targeted by malaria elimination strategies, could substantially reduce malaria transmission in the Amazon. Infected children may remain asymptomatic despite high parasite densities that elicit clinical manifestations in adults.
Funding: US National Institutes of Health, Fundação de Amparo à Pesquisa do Estado de São Paulo, and Belgium Development Cooperation.
Keywords: Amazon; Plasmodium vivax; asymptomatic infections; fever threshold; malaria; sub-patent infections.
Conflict of interest statement
MUF receives a research fellowship from the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Brazil, and was supported by a visiting scientist fellowship from the Casa da América Latina and Fundação Millennium BCP, Portugal. RMC was supported by a PhD scholarship from CNPq. ARA is supported by a postdoctoral scholarship from the Fonds de la Recherche Scientifique (FNRS), Belgium. All other authors declare no competing interests.
Figures

References
-
- Ferreira MU, Castro MC. Malaria situation in Latin America and the Caribbean: residual and resurgent transmission and challenges for control and elimination. Methods Mol Biol. 2019;2013:57–70. - PubMed
-
- World Health Organization. World Malaria Report 2020. Geneva, World Health Organization; 2020. Available at: https://www.who.int/publications/i/item/9789240015791.
-
- Lindblade KA, Steinhardt L, Samuels A, Kachur SP, Slutsker L. The silent threat: asymptomatic parasitemia and malaria transmission. Expert Rev Anti Infect Ther. 2013;11:623–636. - PubMed
-
- Bousema T, Okell L, Felger I, Drakeley C. Asymptomatic malaria infections: detectability, transmissibility and public health relevance. Nat Rev Microbiol. 2014;12:833–840. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
