

Impact Of Prepregnancy Overweight And Obesity On Treatment Modality And Pregnancy Outcome In Women With Gestational Diabetes Mellitus
- PMID: 35663318
- PMCID: PMC9160363
- DOI: 10.3389/fendo.2022.799625
Impact Of Prepregnancy Overweight And Obesity On Treatment Modality And Pregnancy Outcome In Women With Gestational Diabetes Mellitus
Abstract
Background: We aim to evaluate the impact of prepregnancy overweight on treatment modalities of Gestational Diabetes Mellitus (GDM). We assessed the association of increased pregravid Body Mass Index (BMI) with dosing of basal and rapid acting insulin as well as pregnancy outcome.
Methods: We included 509 gestational diabetic women (normal weight: 200, overweight: 157, obese: 152), attending the pregnancy outpatient clinic at the Department of Obstetrics and Gynecology, Medical University of Vienna, in this retrospective study. We used a prospectively compiled database to assess patient characteristics, treatment approaches - particularly maximum doses of basal and rapid acting insulin or metformin - and pregnancy outcome.
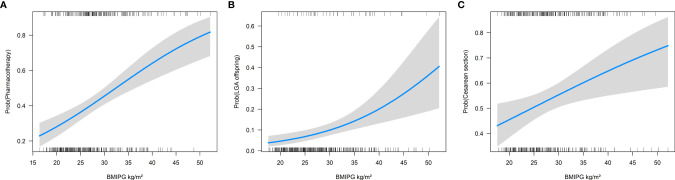
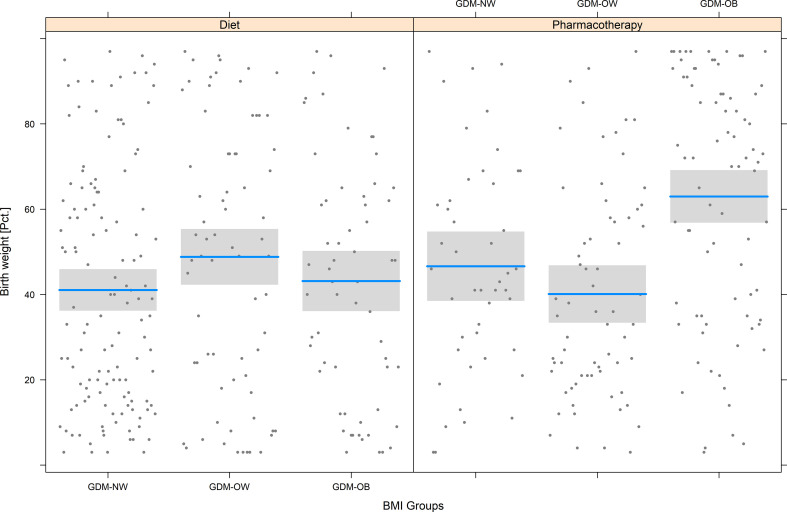
Results: Increased BMI was associated with the need of glucose lowering medication (odds ratio (OR): 1.08 for the increase of 1 kg/m² BMI, 95%CI 1.05-1.11, p<0.001). Mothers with pregestational obesity received the highest amount of insulin. Metformin was more often used in patients with obesity who also required higher daily doses. Maternal BMI was associated with increased risk of cesarean section (OR 1.04, 95%CI 1.01-1.07, p<0.001) and delivering large for gestational age offspring (OR 1.09, 95%CI 1.04-1.13, p<0.001). Birthweight percentiles were highest in patients with obesity who required glucose lowering therapy.
Conclusions: Treatment modalities and outcome in GDM pregnancies are closely related to the extent of maternal BMI. Patients with obesity required glucose lowering medication more often and were at higher risk of adverse pregnancy outcomes. It is crucial to further explore the underlying pathophysiologic mechanisms to optimize clinical management and individual treatment approaches.
Keywords: birth weight; gestational diabetes (GDM); obesity; pharmacotherapy; pregnancy outcome.
Copyright © 2022 Linder, Eder, Monod, Rosicky, Eppel, Redling, Geissler, Huhn, Hösli and Göbl.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Wexler DJ, Powe CE, Barbour LA, Buchanan T, Coustan DR, Corcoy R, et al. . Research Gaps in Gestational Diabetes Mellitus: Executive Summary of a National Institute of Diabetes and Digestive and Kidney Diseases Workshop. Obstetrics Gynecol (2018) 132:496–505. doi: 10.1097/AOG.0000000000002726 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources