

Pulmonary artery-bronchus fistula treated with coil embolization
- PMID: 35663813
- PMCID: PMC9160411
- DOI: 10.1016/j.radcr.2022.04.055
Pulmonary artery-bronchus fistula treated with coil embolization
Abstract
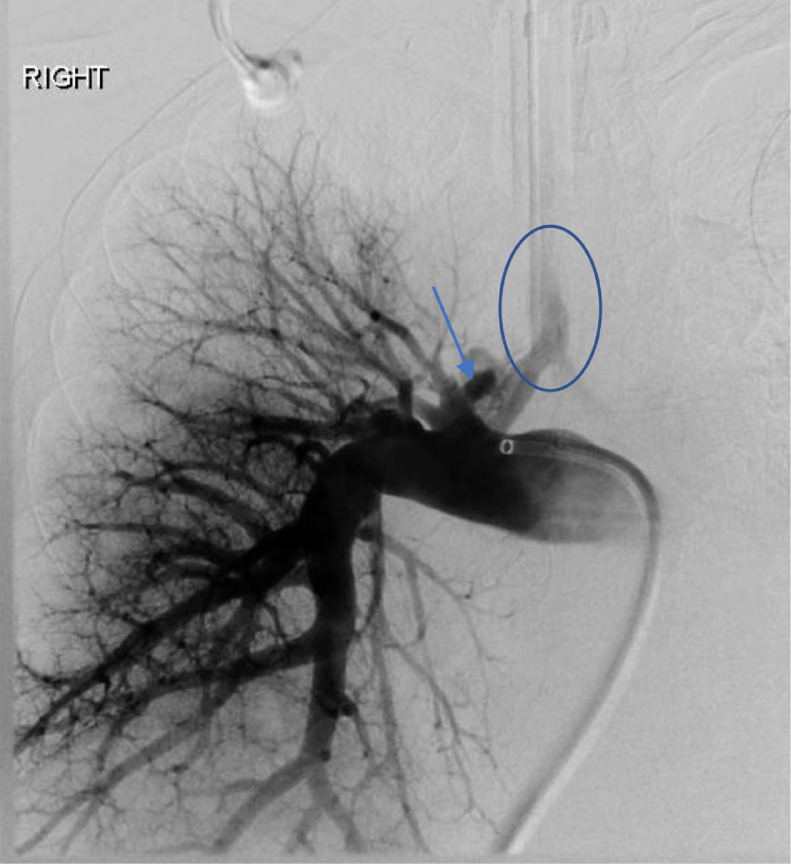
Bronchopulmonary arterial fistula consists of an abnormal connection between the bronchus and the vascular tree and is a rare but serious complication associated with a variety of lung interventions. We present a case of a 61-year-old female with a history of metastatic breast cancer treated with lumpectomy and radiation 20 years prior, who was found to have a fistula between the right pulmonary artery and the right mainstem bronchus. Our patient was treated endovascularly with coil embolization in the setting of massive hemoptysis flooding the trachea, which was successful in controlling the acute bleed, although care was withdrawn in the following days following a discussion with the family given the presence of advanced metastatic disease. This case illustrates the use of endovascular techniques to treat an actively bleeding bronchopulmonary arterial fistulae, including a review of the existing literature regarding the optimal endovascular management strategy. Although our patient did not achieve the best outcome, endovascular intervention with stent-placement or embolization can serve to temporarily halt blood flow through the fistula, stabilizing the patient and allowing for more radical therapy after improvement.
Keywords: BPAF, bronchopulmonary arterial fistula; Bronchopulmonary arterial fistula; Bronchovascular fistula; Coil embolization; DSA, digital subtraction angiogram; Endobronchial stent; IP, interventional pulmonologist; RMB, right mainstem bronchus; RPA, right pulmonary artery; RPA-TA, right pulmonary artery-truncus anterior; RUL, right upper lobe; SEMS, self-expanding metallic stent.
© 2022 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures



References
-
- Santacruz Jose Fernando, Mehta Atul C. Airway complications and management after lung transplantation: ischemia, dehiscence, and stenosis. Proc Am Thoracic Soc. 2009;6(1):79–93. - PubMed
-
- Hoff Steven J., Johnson Joyce E., Frist William H. Aortobronchial fistula after unilateral lung transplantation. Ann Thoracic Surg. 1993;56(6):1402–1403. - PubMed
-
- Murthy SC, Blackstone EH, Gildea TR, et al. Impact of anastomotic airway complications after lung transplantation. Ann Thorac Surg. 2007;84(2):401–409. Aug409.e1-4. doi: 10.1016/j.athoracsur.2007.05.018. PMID: 17643606. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
