

Antibiotic-resistant organisms establish reservoirs in new hospital built environments and are related to patient blood infection isolates
- PMID: 35664456
- PMCID: PMC9160058
- DOI: 10.1038/s43856-022-00124-5
Antibiotic-resistant organisms establish reservoirs in new hospital built environments and are related to patient blood infection isolates
Abstract
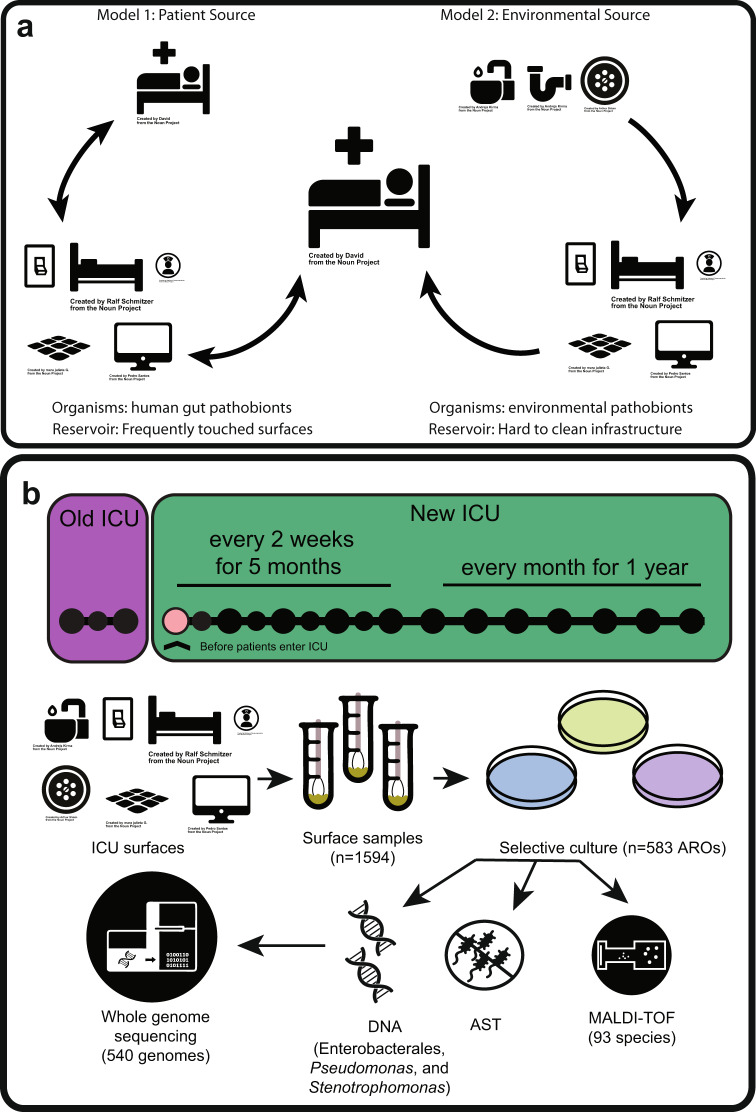
Background: Healthcare-associated infections due to antibiotic-resistant organisms pose an acute and rising threat to critically ill and immunocompromised patients. To evaluate reservoirs of antibiotic-resistant organisms as a source of transmission to patients, we interrogated isolates from environmental surfaces, patient feces, and patient blood infections from an established and a newly built intensive care unit.
Methods: We used selective culture to recover 829 antibiotic-resistant organisms from 1594 environmental and 72 patient fecal samples, in addition to 81 isolates from blood cultures. We conducted antibiotic susceptibility testing and short- and long-read whole genome sequencing on recovered isolates.
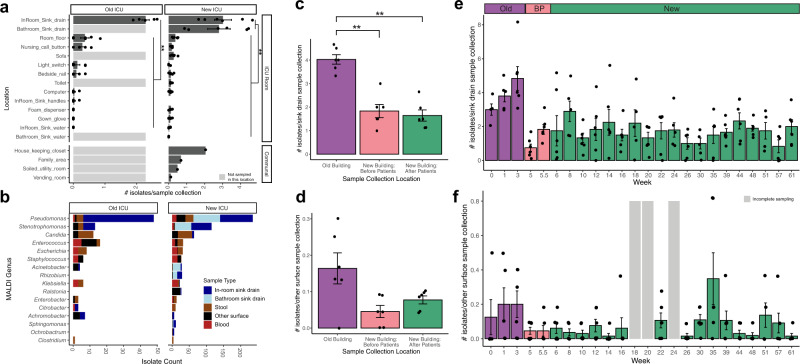
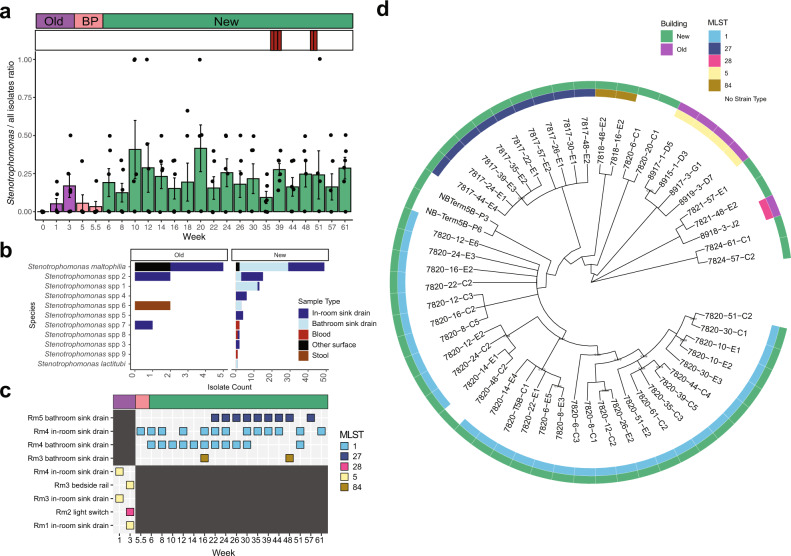
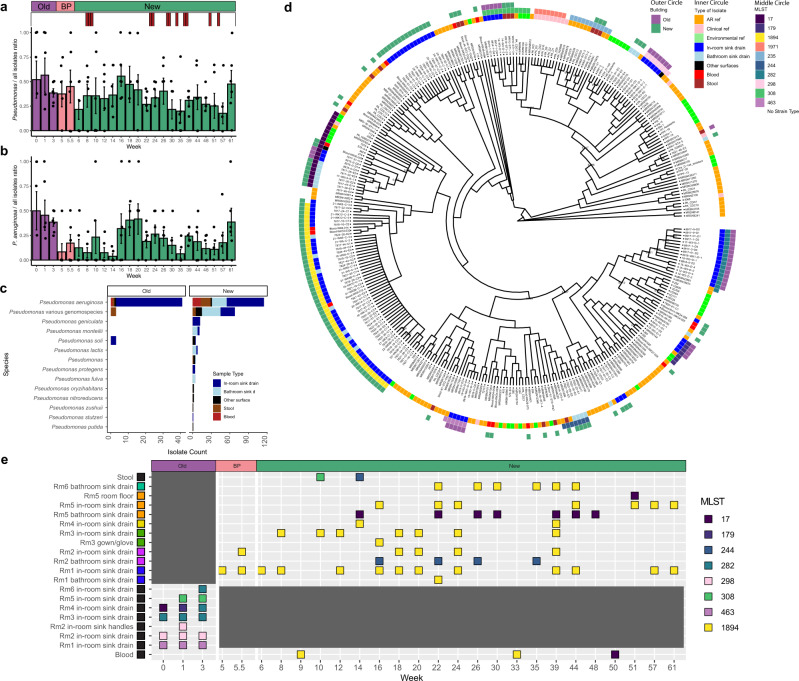
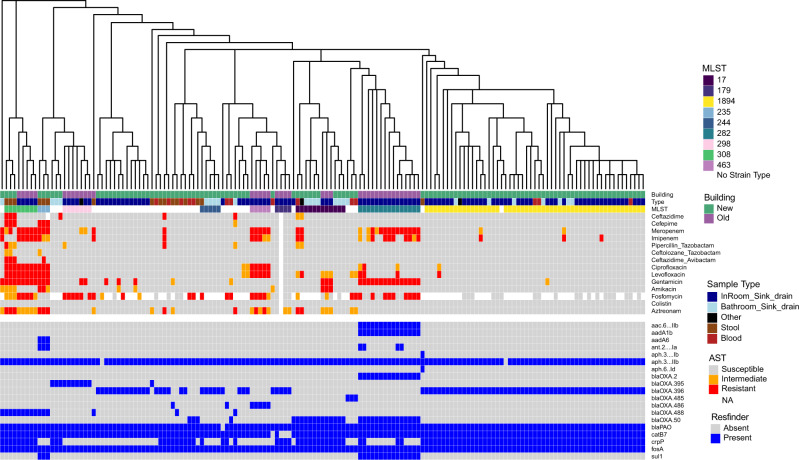
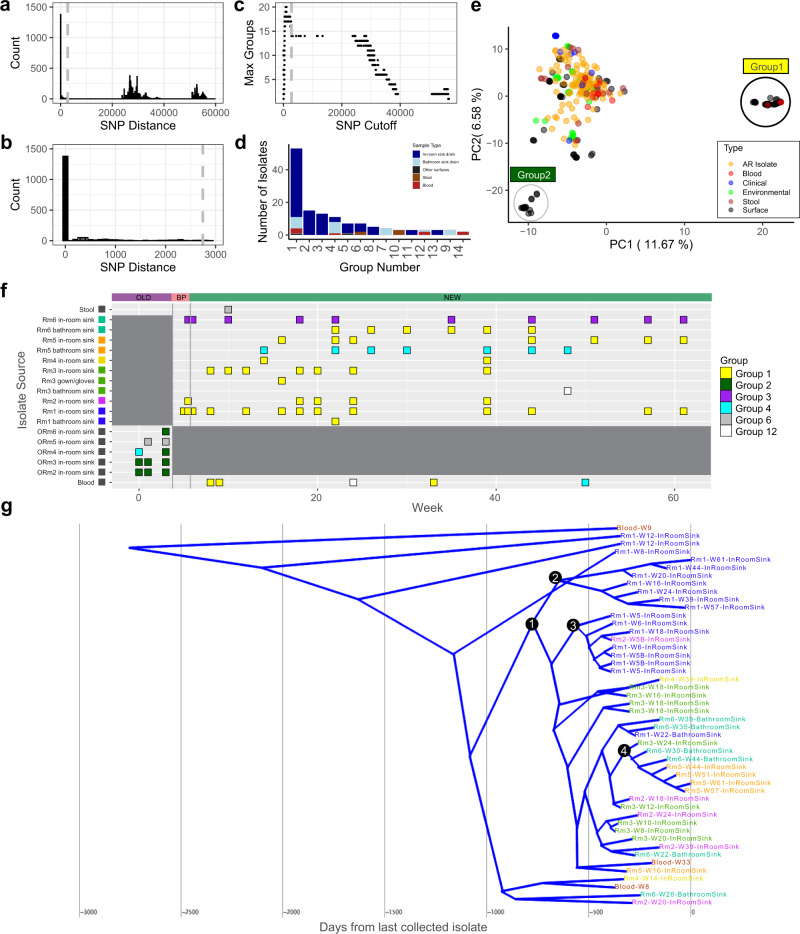
Results: Antibiotic-resistant organism burden is highest in sink drains compared to other surfaces. Pseudomonas aeruginosa is the most frequently cultured organism from surfaces in both intensive care units. From whole genome sequencing, different lineages of P. aeruginosa dominate in each unit; one P. aeruginosa lineage of ST1894 is found in multiple sink drains in the new intensive care unit and 3.7% of blood isolates analyzed, suggesting movement of this clone between the environment and patients.
Conclusions: These results highlight antibiotic-resistant organism reservoirs in hospital built environments as an important target for infection prevention in hospitalized patients.
Keywords: Antimicrobial resistance; Comparative genomics; Disease prevention; Genetic variation; Infectious-disease epidemiology.
© The Author(s) 2022.
Conflict of interest statement
Competing interestsThe authors declare no competing interests.
Figures
References
-
- Rosenthal VD, Guzman S, Migone O, Crnich CJ. The attributable cost, length of hospital stay, and mortality of central line-associated bloodstream infection in intensive care departments in Argentina: a prospective, matched analysis. Am. J. Infect. Control. 2003;31:475–480. doi: 10.1016/j.ajic.2003.03.002. - DOI - PubMed
-
- Giraldi G, Montesano M, Sandorfi F, Iachini M, Orsi GB. Excess length of hospital stay due to healthcare acquired infections: methodologies evaluation. Ann. Ig. 2019;31:507–516. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
