Generative models for reproducible coronary calcium scoring
- PMID: 35664539
- PMCID: PMC9154523
- DOI: 10.1117/1.JMI.9.5.052406
Generative models for reproducible coronary calcium scoring
Abstract
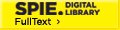
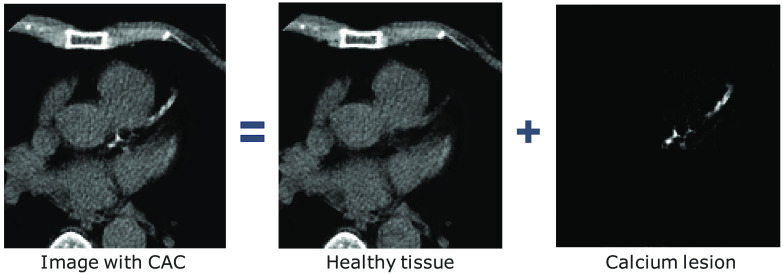
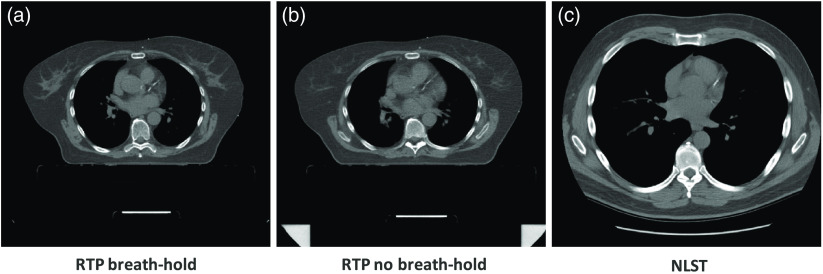
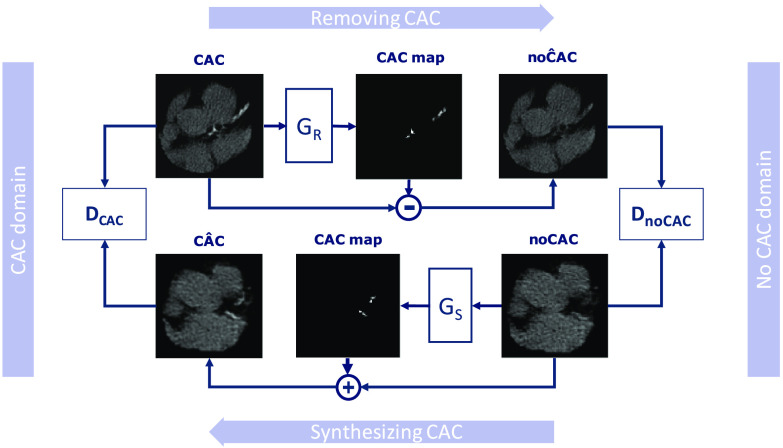
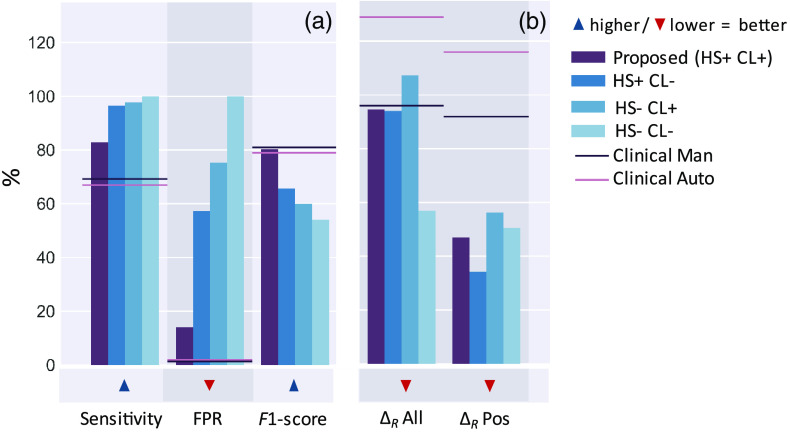
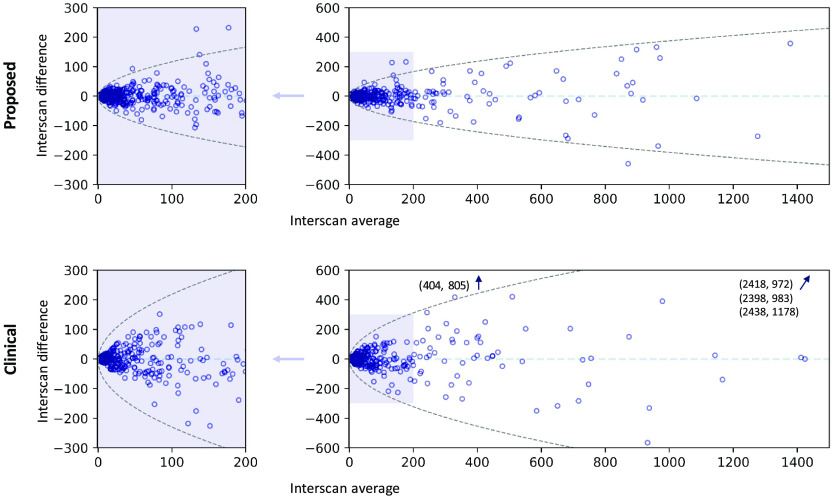
Purpose: Coronary artery calcium (CAC) score, i.e., the amount of CAC quantified in CT, is a strong and independent predictor of coronary heart disease (CHD) events. However, CAC scoring suffers from limited interscan reproducibility, which is mainly due to the clinical definition requiring application of a fixed intensity level threshold for segmentation of calcifications. This limitation is especially pronounced in non-electrocardiogram-synchronized computed tomography (CT) where lesions are more impacted by cardiac motion and partial volume effects. Therefore, we propose a CAC quantification method that does not require a threshold for segmentation of CAC. Approach: Our method utilizes a generative adversarial network (GAN) where a CT with CAC is decomposed into an image without CAC and an image showing only CAC. The method, using a cycle-consistent GAN, was trained using 626 low-dose chest CTs and 514 radiotherapy treatment planning (RTP) CTs. Interscan reproducibility was compared to clinical calcium scoring in RTP CTs of 1662 patients, each having two scans. Results: A lower relative interscan difference in CAC mass was achieved by the proposed method: 47% compared to 89% manual clinical calcium scoring. The intraclass correlation coefficient of Agatston scores was 0.96 for the proposed method compared to 0.91 for automatic clinical calcium scoring. Conclusions: The increased interscan reproducibility achieved by our method may lead to increased reliability of CHD risk categorization and improved accuracy of CHD event prediction.
Keywords: calcium scoring; computed tomography; cycle-consistent generative adversarial network; generative models; reproducibility.
© 2022 Society of Photo-Optical Instrumentation Engineers (SPIE).
Figures
Similar articles
-
Automatic Coronary Artery Calcium Scoring on Radiotherapy Planning CT Scans of Breast Cancer Patients: Reproducibility and Association with Traditional Cardiovascular Risk Factors.PLoS One. 2016 Dec 9;11(12):e0167925. doi: 10.1371/journal.pone.0167925. eCollection 2016. PLoS One. 2016. PMID: 27936125 Free PMC article.
-
Impact of automatically detected motion artifacts on coronary calcium scoring in chest computed tomography.J Med Imaging (Bellingham). 2018 Oct;5(4):044007. doi: 10.1117/1.JMI.5.4.044007. Epub 2018 Dec 11. J Med Imaging (Bellingham). 2018. PMID: 30840743 Free PMC article.
-
Automated coronary artery calcification scoring in non-gated chest CT: agreement and reliability.PLoS One. 2014 Mar 13;9(3):e91239. doi: 10.1371/journal.pone.0091239. eCollection 2014. PLoS One. 2014. PMID: 24625525 Free PMC article.
-
Extracoronary Thoracic and Coronary Artery Calcifications on Chest CT for Lung Cancer Screening: Association with Established Cardiovascular Risk Factors - The "CT-Risk" Trial.Acad Radiol. 2015 Jul;22(7):880-9. doi: 10.1016/j.acra.2015.03.005. Epub 2015 May 7. Acad Radiol. 2015. PMID: 25957500 Review.
-
Scoring of coronary artery calcium scans: history, assumptions, current limitations, and future directions.Atherosclerosis. 2015 Mar;239(1):109-17. doi: 10.1016/j.atherosclerosis.2014.12.040. Epub 2015 Jan 2. Atherosclerosis. 2015. PMID: 25585030 Review.
Cited by
-
Automated cardiovascular risk categorization through AI-driven coronary calcium quantification in cardiac PET acquired attenuation correction CT.J Nucl Cardiol. 2023 Jun;30(3):955-969. doi: 10.1007/s12350-022-03047-9. Epub 2022 Jul 18. J Nucl Cardiol. 2023. PMID: 35851642 Free PMC article.
-
Finetuned Super-Resolution Generative Adversarial Network (Artificial Intelligence) Model for Calcium Deblooming in Coronary Computed Tomography Angiography.J Pers Med. 2022 Aug 23;12(9):1354. doi: 10.3390/jpm12091354. J Pers Med. 2022. PMID: 36143139 Free PMC article.
-
Special Section Guest Editorial: Advances in High-Dimensional Medical Image Processing.J Med Imaging (Bellingham). 2022 Sep;9(5):052401. doi: 10.1117/1.JMI.9.5.052401. Epub 2022 Oct 31. J Med Imaging (Bellingham). 2022. PMID: 36330041 Free PMC article.
References
-
- Wang H., et al. , “Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the global burden of disease study 2015,” The Lancet 388(10053), 1459–1544 (2016).LANCAO10.1016/S0140-6736(16)31012-1 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials