

LUtarjet-limit unique coracoid osteotomy Latarjet (With video)
- PMID: 35664892
- PMCID: PMC9155144
- DOI: 10.1093/burnst/tkac021
LUtarjet-limit unique coracoid osteotomy Latarjet (With video)
Abstract
Background: The Latarjet procedure is an effective technique for the treatment of recurrent anterior shoulder dislocation with glenoid bone loss. However, the inevitable destruction of the coracoacromial arch may result in humeral head translation. The aim of the study is to introduce a modified Latarjet technique with coracoacromial arch preservation as well as its short term clinical outcomes.
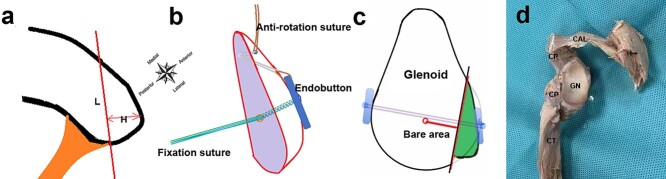
Methods: We propose a novel individualized flexible arthroscopic suture button fixation Latarjet technique called `LUtarjet' with video. Precise measurements of the coracoid process, glenoid deficiency and osteotomy plane were made preoperatively. Only three arthroscopic portals were needed and limit unique coracoid osteotomy was performed with coracoacromial arch preservation. The mini window splitting of the subscapularis was performed from the posterior to the anterior direction and the split window was as small as 8-10 mm in length.
Results: A total of 27 patients (25.6 ± 5.4 years) were included in the study. The average surgical duration was 55.6 ± 6.3 min and the mean follow-up time was 8.1 ± 1.5 months. The functional score was significantly improved at the last follow-up. Radiologic evidence showed that the bone graft healing was placed in the desired position. No complications were found.
Conclusions: We present a fast, easy, accurate, safe arthroscopic 'LUtarjet' technique called FEAST that can simplify the arthroscopic Latarjet process and achieve a satisfactory bone graft position and satisfactory short-term clinical outcomes.
Level of evidence: IV, case series.
Keywords: Coracoacromial archBackground; Glenoid bone loss; Latarjet; Recurrent anterior shoulder dislocation; Suture button fixation.
© The Author(s) 2022. Published by Oxford University Press.
Figures








Similar articles
-
[Anatomical study of the limited osteotomy suture button fixation Latarjet procedure with coracoacromial ligament preservation].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024 Jun 15;38(6):691-695. doi: 10.7507/1002-1892.202403123. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024. PMID: 38918189 Free PMC article. Chinese.
-
Arthroscopic Cortical-Button Latarjet Procedure for Anterior Shoulder Instability With Glenoid Bone Loss.Video J Sports Med. 2022 Mar 15;2(2):26350254211038337. doi: 10.1177/26350254211038337. eCollection 2022 Mar-Apr. Video J Sports Med. 2022. PMID: 40308466 Free PMC article.
-
[Early-term effectiveness of Latarjet procedure by coracoid osteotomy with preserving coracoacromial ligament for recurrent anterior shoulder dislocation].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024 Jun 15;38(6):655-659. doi: 10.7507/1002-1892.202403108. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024. PMID: 38918183 Free PMC article. Chinese.
-
[Development and research progress of suture button fixation Latarjet procedure].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024 Jun 15;38(6):635-640. doi: 10.7507/1002-1892.202404031. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024. PMID: 38918180 Free PMC article. Review. Chinese.
-
Arthroscopic Bankart-Bristow-Latarjet (2B3) Procedure: How to Do It and Tricks To Make it Easier and Safe.Orthop Clin North Am. 2010 Jul;41(3):381-92. doi: 10.1016/j.ocl.2010.03.005. Orthop Clin North Am. 2010. PMID: 20497813 Review.
Cited by
-
Mechanistic study of the effect of flexible fixation and load-bearing stress environment on fracture healing and shaping.Animal Model Exp Med. 2024 Dec;7(6):816-823. doi: 10.1002/ame2.12448. Epub 2024 Jul 8. Animal Model Exp Med. 2024. PMID: 38978345 Free PMC article.
-
[Anatomical study of the limited osteotomy suture button fixation Latarjet procedure with coracoacromial ligament preservation].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024 Jun 15;38(6):691-695. doi: 10.7507/1002-1892.202403123. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024. PMID: 38918189 Free PMC article. Chinese.
-
[Modified Latarjet splitting subscapularis muscle under arthroscopy: an anatomical study based on axillary nerve, glenoid, and subscapularis muscle].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023 May 15;37(5):556-560. doi: 10.7507/1002-1892.202302059. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023. PMID: 37190831 Free PMC article. Chinese.
-
Modified Suture Button Latarjet Procedure With Coracoacromial Ligament and Pectoralis Minor Preservation: An Approach to Avoid Subscapularis Split.Arthrosc Tech. 2024 Sep 23;14(3):103251. doi: 10.1016/j.eats.2024.103251. eCollection 2025 Mar. Arthrosc Tech. 2024. PMID: 40207328 Free PMC article.
-
[Mid-term effectiveness of LU-tarjet procedure for recurrent anterior shoulder dislocation].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024 Jun 15;38(6):646-654. doi: 10.7507/1002-1892.202404058. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024. PMID: 38918182 Free PMC article. Chinese.
References
-
- Latarjet M. Treatment of recurrent dislocation of the shoulder. Lyon Chir. 1954;49:994–7. - PubMed
-
- Walch G, Charret P, Pietro-Paoli H, Dejour H. Anterior recurrent luxation of the shoulder. Postoperative recurrences. Rev Chir Orthop Reparatrice Appar Mot. 1986;72:541–55. - PubMed
-
- Joshi MA, Young AA, Balestro JC, Walch G. The Latarjet-Patte procedure for recurrent anterior shoulder instability in contact athletes. Clin Sports Med. 2013;32:731–9. - PubMed
-
- Giles JW, Boons HW, Elkinson I, Faber KJ, Ferreira LM, Johnson JA, et al. Does the dynamic sling effect of the Latarjet procedure improve shoulder stability? A biomechanical evaluation. J Shoulder Elb Surg. 2013;22:821–7. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
