

Medication-Related Osteonecrosis of the Jaw in Patients Treated Concurrently with Antiresorptive and Antiangiogenic Agents: Systematic Review and Meta-Analysis
- PMID: 35665023
- PMCID: PMC9138478
- DOI: 10.36401/JIPO-21-14
Medication-Related Osteonecrosis of the Jaw in Patients Treated Concurrently with Antiresorptive and Antiangiogenic Agents: Systematic Review and Meta-Analysis
Abstract
Introduction: Medication-related osteonecrosis of the jaws (MRONJ) is a known adverse event related to the use of antiresorptive (AR) drugs. More recently, an association between antiangiogenic (AA) drugs and MRONJ has been suggested. This review aimed to investigate the overall prevalence and relative risk of MRONJ in patients treated concurrently with AA and AR agents in comparison with a single AA or AR drug.
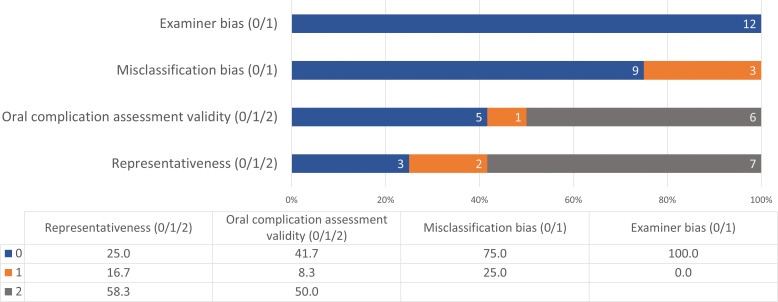
Methods: A review protocol was registered with PROSPERO (ID: CRD42020214244). A systematic literature search, study selection, quality assessment, and data extraction were carried out following PRISMA guidelines. Random-effects meta-analysis models were used to summarize relative estimates for the outcomes, namely prevalence and relative risk of MRONJ. Exposure variable included type of drug, specifically AA and AR agents administered either concurrently or individually.
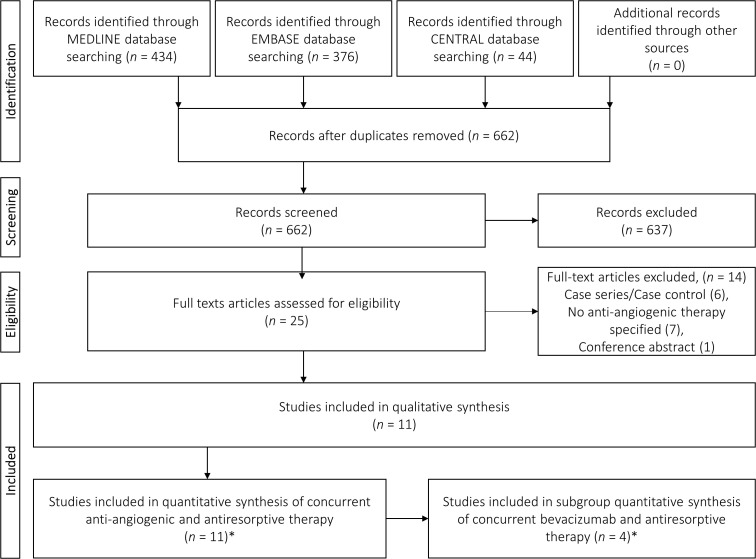
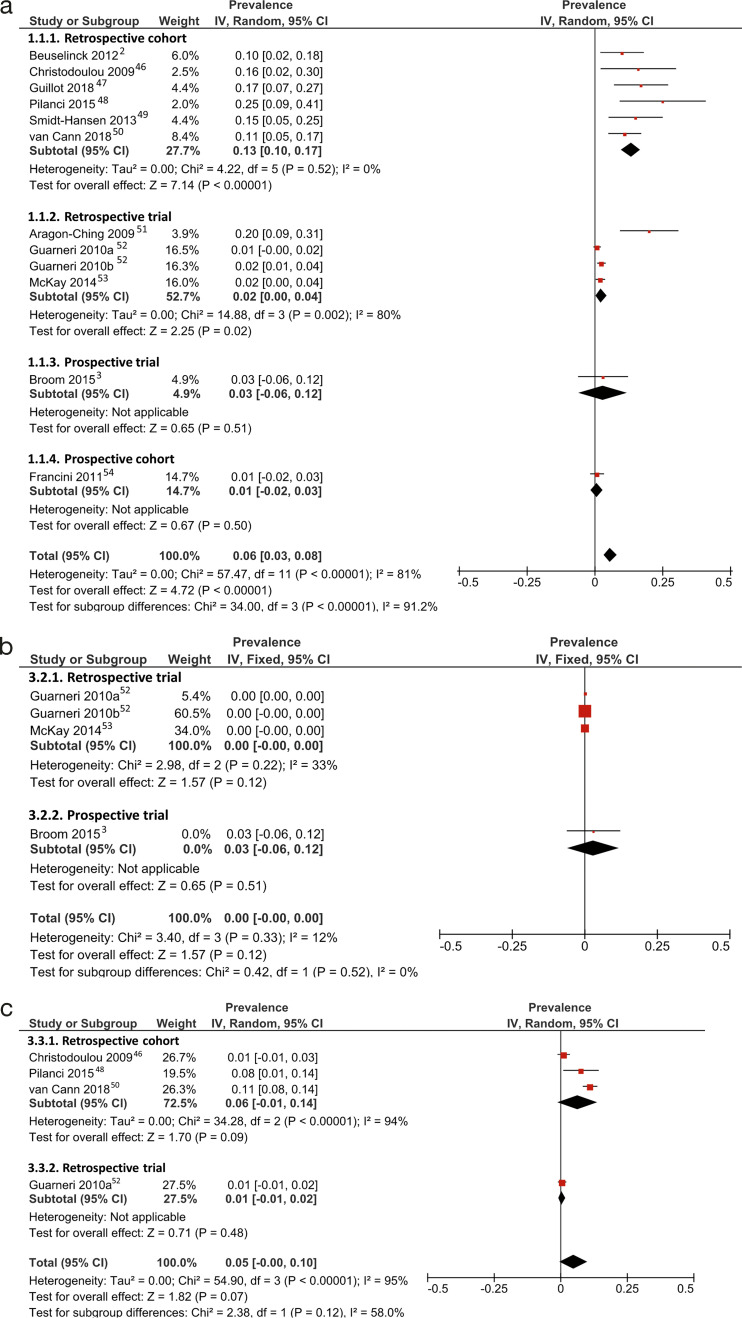
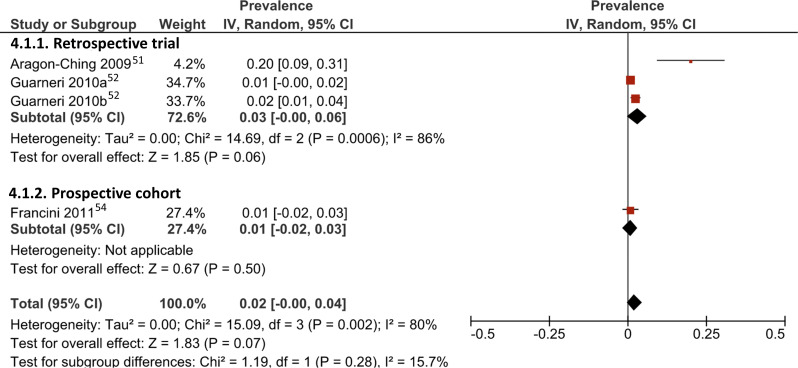
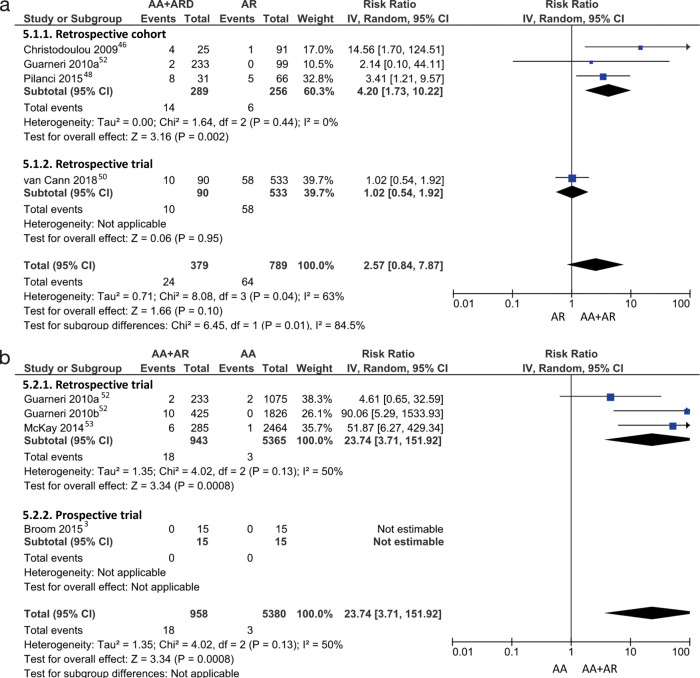
Results: Eleven studies were included in the final qualitative and quantitative syntheses. The overall pooled weighted prevalence of MRONJ with concurrent AA-AR drugs was 6% (95% CI: 3-8%), compared with 0% (95% CI: 0-0%) for AA only and 5% (95% CI: 0-10%) for AR only. However, high heterogeneity was noted among included studies. Retrospective cohort studies showed a higher pooled prevalence of 13% (95% CI: 10-17%) for concurrent AA-AR therapy. The pooled risk ratio for MRONJ revealed a risk with concurrent AA-AR drugs 2.57 times as high as with AR only (95% CI: 0.84-7.87); however, this difference was not statistically significant. Concurrent AA-AR drugs had a risk for MRONJ 23.74 times as high as with AA only (95% CI: 3.71-151.92).
Conclusions: High-quality, representative studies are needed for accurate estimation of relative risk of MRONJ with concurrent AA and AR therapy.
Keywords: antiangiogenic drugs; antiresorptive drugs; bisphosphonates; denosumab; osteonecrosis.
Conflict of interest statement
Conflict of Interest: None.
Figures
References
-
- Broom RJ, Hinder V, Sharples K, et al. Everolimus and zoledronic acid in patients with renal cell carcinoma with bone metastases: a randomized first-line phase II trial. Clin Genitourin Cancer . 2015;13:50–58. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials