

Rituximab abrogates aquaporin-4-specific germinal center activity in patients with neuromyelitis optica spectrum disorders
- PMID: 35666871
- PMCID: PMC9214492
- DOI: 10.1073/pnas.2121804119
Rituximab abrogates aquaporin-4-specific germinal center activity in patients with neuromyelitis optica spectrum disorders
Abstract
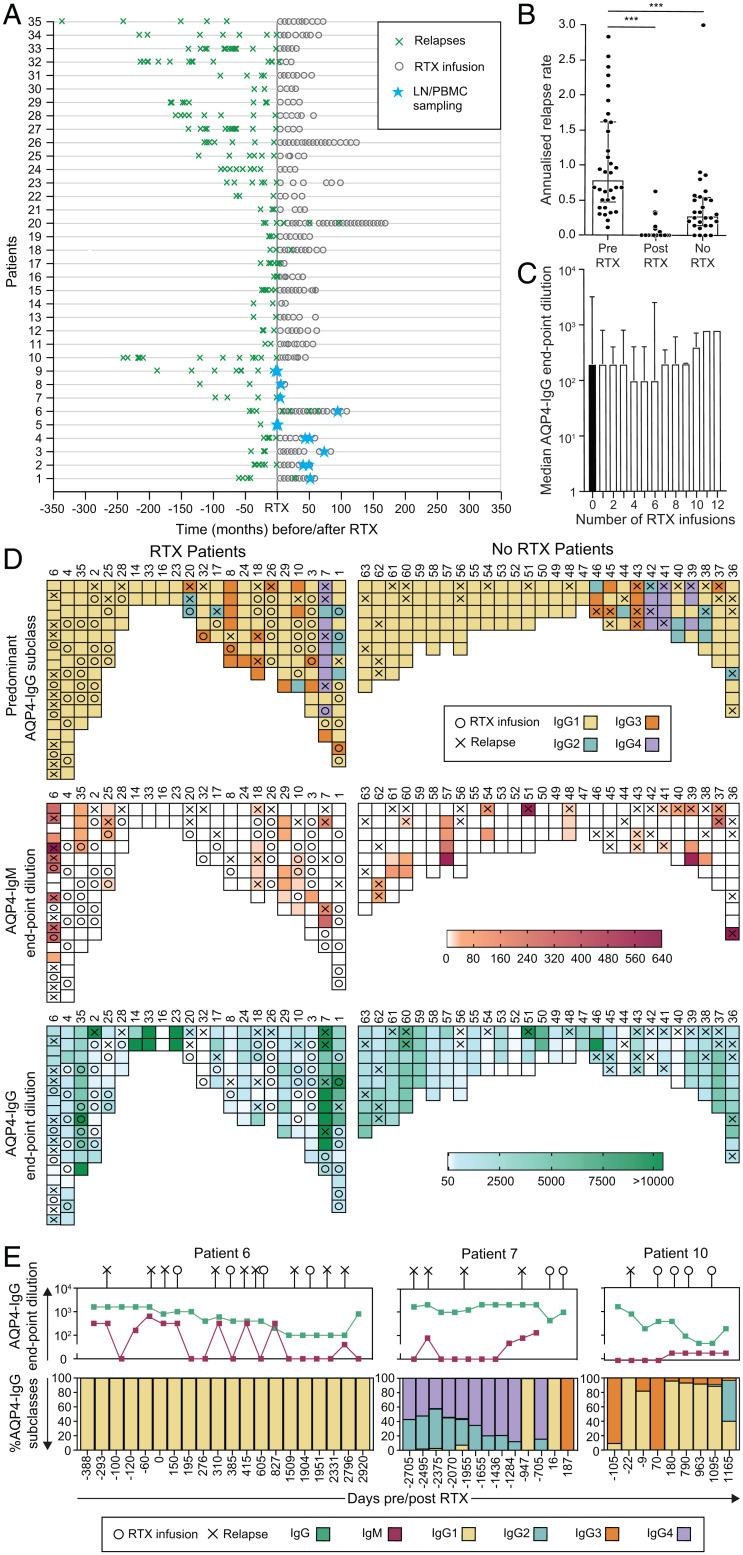
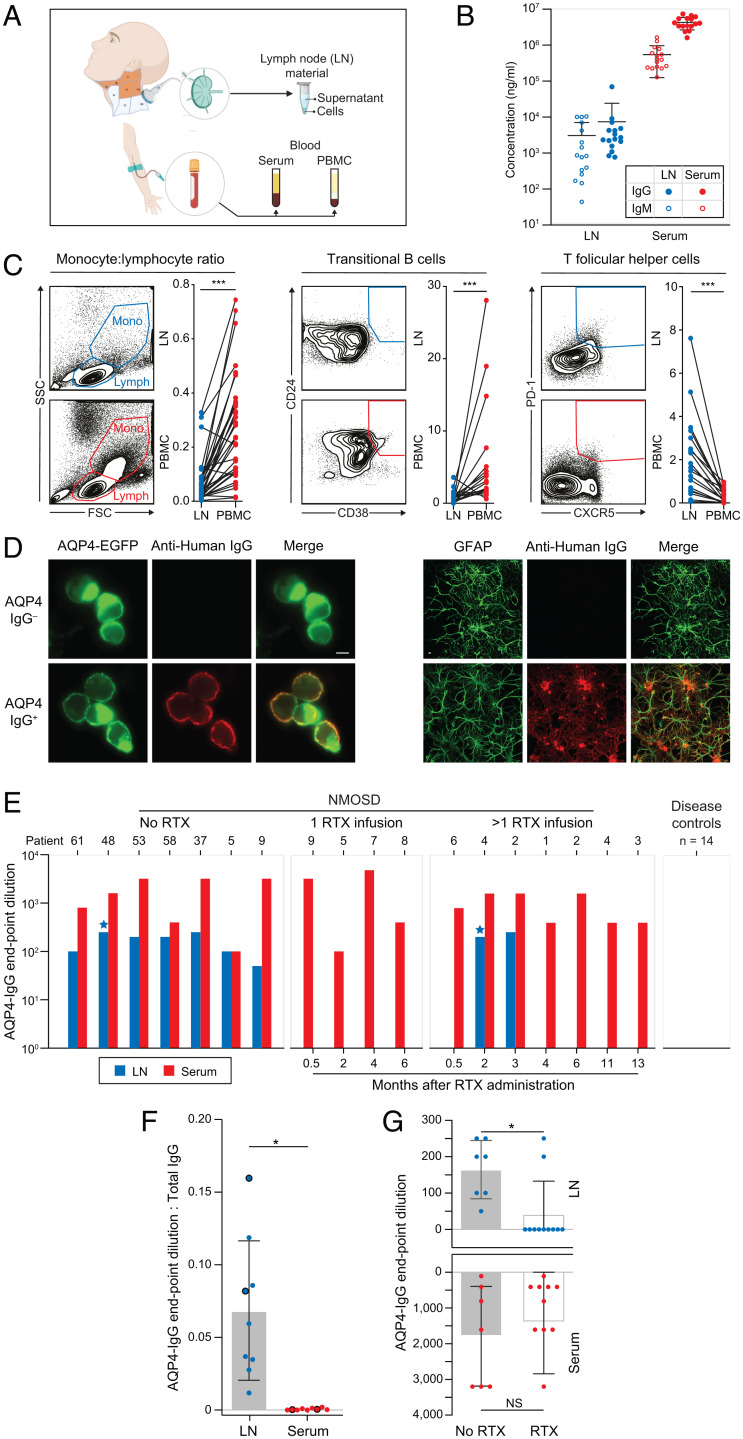
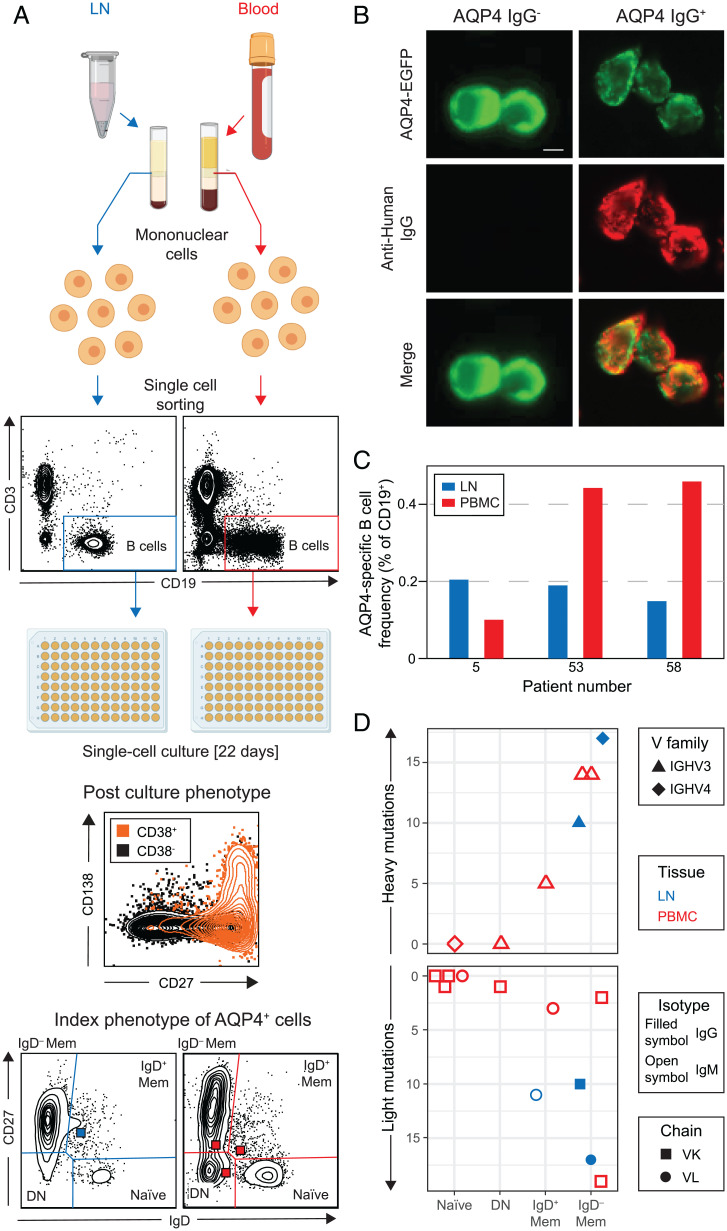
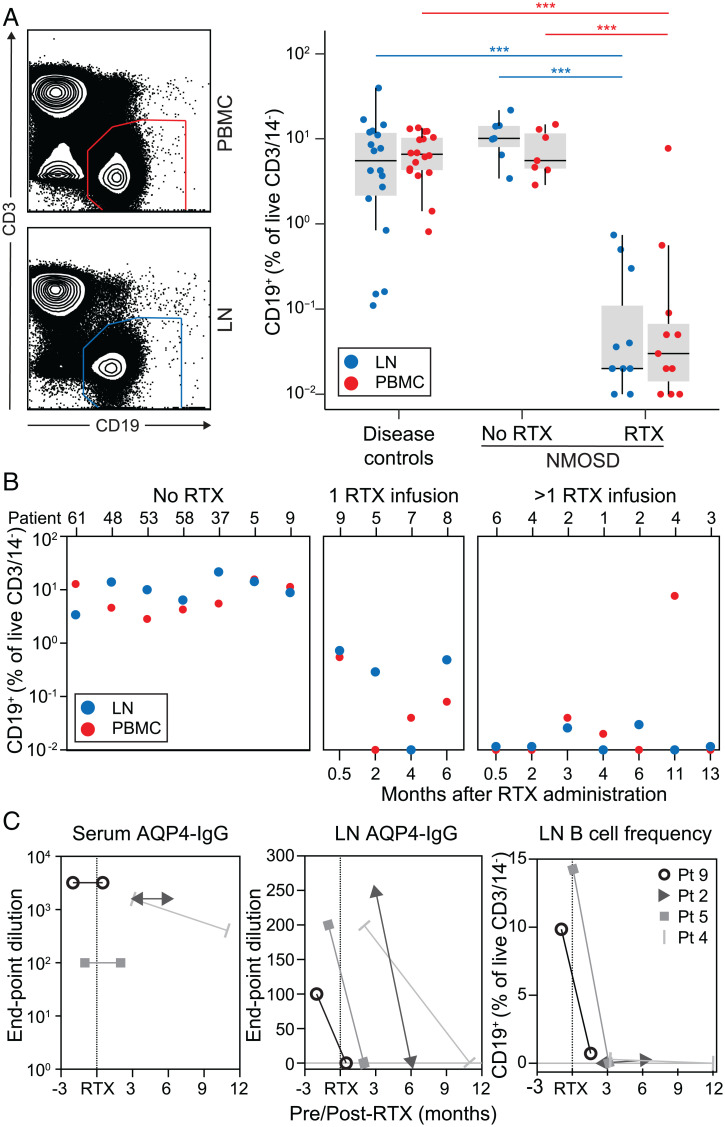
Neuromyelitis optica spectrum disorders (NMOSDs) are caused by immunoglobulin G (IgG) autoantibodies directed against the water channel aquaporin-4 (AQP4). In NMOSDs, discrete clinical relapses lead to disability and are robustly prevented by the anti-CD20 therapeutic rituximab; however, its mechanism of action in autoantibody-mediated disorders remains poorly understood. We hypothesized that AQP4-IgG production in germinal centers (GCs) was a core feature of NMOSDs and could be terminated by rituximab. To investigate this directly, deep cervical lymph node (dCLN) aspirates (n = 36) and blood (n = 406) were studied in a total of 63 NMOSD patients. Clinical relapses were associated with AQP4-IgM generation or shifts in AQP4-IgG subclasses (odds ratio = 6.0; range of 3.3 to 10.8; P < 0.0001), features consistent with GC activity. From seven dCLN aspirates of patients not administered rituximab, AQP4-IgGs were detected alongside specific intranodal synthesis of AQP4-IgG. AQP4-reactive B cells were isolated from unmutated naive and mutated memory populations in both blood and dCLNs. After rituximab administration, fewer clinical relapses (annual relapse rate of 0.79 to 0; P < 0.001) were accompanied by marked reductions in both AQP4-IgG (fourfold; P = 0.004) and intranodal B cells (430-fold; P < 0.0001) from 11 dCLNs. Our findings implicate ongoing GC activity as a rituximab-sensitive driver of AQP4 antibody production. They may explain rituximab’s clinical efficacy in several autoantibody-mediated diseases and highlight the potential value of direct GC measurements across autoimmune conditions.
Keywords: aquaporin; autoimmunity; cervical lymph nodes; neuromyelitis optica; rituximab.
Conflict of interest statement
Competing interest statement: S.R.I. is supported by the Medical Research Council (MR/V007173/1), Wellcome Trust (104079/Z/14/Z), BMA Research Grants - 2013 Vera Down grant, Epilepsy Research UK (P1201), and the Fulbright UK-US commission (MS-Research Society Award). This research was funded in whole, or in part, by the Wellcome Trust (grant number 104079/Z/14/Z). For the purpose of Open Access, the author has applied a CC BY public copyright license to any Author Accepted Manuscript version arising from this submission. J.T. is supported by the Swedish Wenner-Gren foundations. P.W. is supported by the UK NMO commissioning group. B.S. is supported by the Association of British Neurologists via the Patrick Berthoud Charitable Trust. The work is supported by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre. P.W. and S.R.I. are coapplicants and receive royalties on patent application WO/2010/046716 entitled “Neurological Autoimmune Disorders” (the patent has been licensed for the development of assays for LGI1 and other VGKC-complex antibodies) and have filed two other patents regarding autoantibody diagnostic algorithms.
Figures
References
-
- Lennon V. A., et al. , A serum autoantibody marker of neuromyelitis optica: Distinction from multiple sclerosis. Lancet 364, 2106–2112 (2004). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
