

Vaccination of household chickens results in a shift in young children's diet and improves child growth in rural Kenya
- PMID: 35666875
- PMCID: PMC9214528
- DOI: 10.1073/pnas.2122389119
Vaccination of household chickens results in a shift in young children's diet and improves child growth in rural Kenya
Abstract
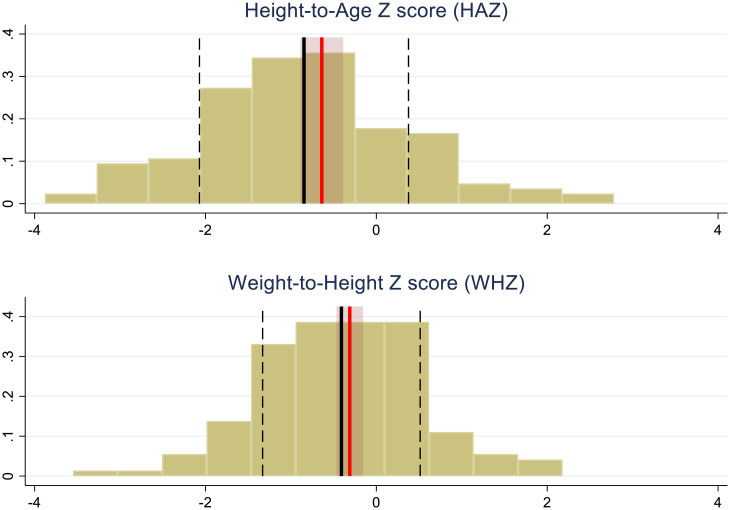
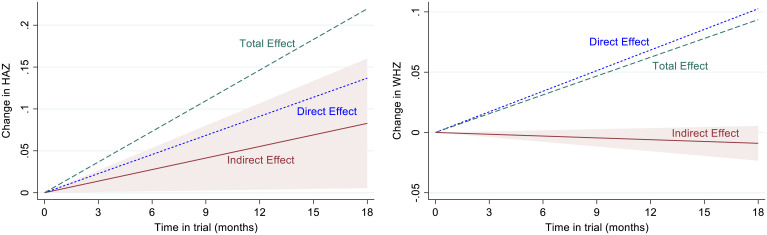
Childhood growth faltering remains unacceptably high in sub-Saharan Africa. Rural communities dependent on household food production with limited off-farm income or liquid assets to bridge seasonal food availability are especially vulnerable. A cross-sectional survey in Siaya County, Kenya identified 23.5 and 4.8% of children under 5 y of age as stunted and wasted, respectively, using height-for-age Z (HAZ) scores to detect stunting and weight-for-height Z (WHZ) scores for wasting. Although these households are classified as living in poverty or extreme poverty with very limited off-farm income, households commonly have on-farm resources that could be developed to improve nutrition. While 95% of these households have chickens and consumption of eggs was shown to increase childhood growth by an average of 5%, the average flock size is small and constrained by high mortality due to infectious disease. We hypothesized that interventions to relieve this constraint would translate into household decisions influencing the diets and growth of children. Here, we show that vaccination of chickens against Newcastle disease has a causal impact on children’s consumption of animal source foods rich in protein and micronutrients relative to a high-carbohydrate, grain-based diet. Children in treatment households (chicken vaccination) showed overall increases in scores for both HAZ and WHZ relative to control households, benefiting both girls and boys. The findings demonstrate the impact of directing interventions at common on-farm assets managed by women in rural communities and support programs to enhance productivity at the household level.
Keywords: animal source foods; child growth; household decisions; nutrition.
Conflict of interest statement
The authors declare no competing interest.
Figures
Similar articles
-
Impact of routine Newcastle disease vaccination on chicken flock size in smallholder farms in western Kenya.PLoS One. 2021 Mar 18;16(3):e0248596. doi: 10.1371/journal.pone.0248596. eCollection 2021. PLoS One. 2021. PMID: 33735266 Free PMC article.
-
Mortality as the primary constraint to enhancing nutritional and financial gains from poultry: A multi-year longitudinal study of smallholder farmers in western Kenya.PLoS One. 2020 May 29;15(5):e0233691. doi: 10.1371/journal.pone.0233691. eCollection 2020. PLoS One. 2020. PMID: 32470070 Free PMC article.
-
Does Village Chicken-Keeping Contribute to Young Children's Diets and Growth? A Longitudinal Observational Study in Rural Tanzania.Nutrients. 2018 Nov 19;10(11):1799. doi: 10.3390/nu10111799. Nutrients. 2018. PMID: 30463264 Free PMC article.
-
More evidence on cash transfers and child nutritional outcomes: a systematic review and meta-analysis.BMJ Glob Health. 2022 Apr;7(4):e008233. doi: 10.1136/bmjgh-2021-008233. BMJ Glob Health. 2022. PMID: 35365481 Free PMC article.
-
Contribution of Village Chickens in Sustainable and Healthy Food Systems for Children along a Rural-Urban Gradient: A Systematic Review.Foods. 2023 Sep 25;12(19):3553. doi: 10.3390/foods12193553. Foods. 2023. PMID: 37835206 Free PMC article. Review.
Cited by
-
The impact of livestock interventions on nutritional outcomes of children younger than 5 years old and women in Africa: a systematic review and meta-analysis.Front Nutr. 2023 Jul 6;10:1166495. doi: 10.3389/fnut.2023.1166495. eCollection 2023. Front Nutr. 2023. PMID: 37485389 Free PMC article. Review.
-
Economics of East Coast fever: a literature review.Front Vet Sci. 2023 Sep 13;10:1239110. doi: 10.3389/fvets.2023.1239110. eCollection 2023. Front Vet Sci. 2023. PMID: 37771945 Free PMC article. Review.
-
Factors Influencing Iron Levels Among Women of Reproductive Age and Children 6-48 Months in Livestock-Keeping Communities in Narok County, Kenya.Food Sci Nutr. 2025 Jan 22;13(1):e4625. doi: 10.1002/fsn3.4625. eCollection 2025 Jan. Food Sci Nutr. 2025. PMID: 39844793 Free PMC article.
References
-
- World Health Organization, Global nutrition targets 2025 (2014). https://www.who.int/publications/i/item/WHO-NMH-NHD-14.2. Accessed 8 August 2021.
-
- Bloss E., Wainaina F., Bailey R. C., Prevalence and predictors of underweight, stunting, and wasting among children aged 5 and under in western Kenya. J. Trop. Pediatr. 50, 260–270 (2004). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
