

Effect of Molnupiravir on Biomarkers, Respiratory Interventions, and Medical Services in COVID-19 : A Randomized, Placebo-Controlled Trial
- PMID: 35667065
- PMCID: PMC9186515
- DOI: 10.7326/M22-0729
Effect of Molnupiravir on Biomarkers, Respiratory Interventions, and Medical Services in COVID-19 : A Randomized, Placebo-Controlled Trial
Abstract
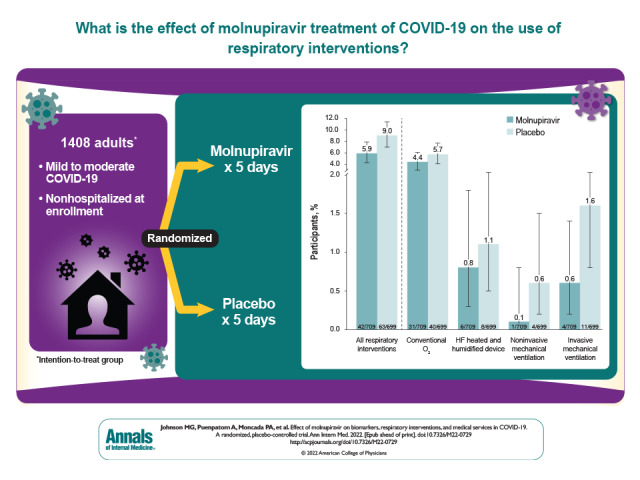
Background: In the MOVe-OUT trial, molnupiravir showed a clinically meaningful reduction in the risk for hospitalization or death in adults with mild to moderate COVID-19 and risk factors for progression to severe disease.
Objective: To identify other potential clinical benefits of molnupiravir versus placebo.
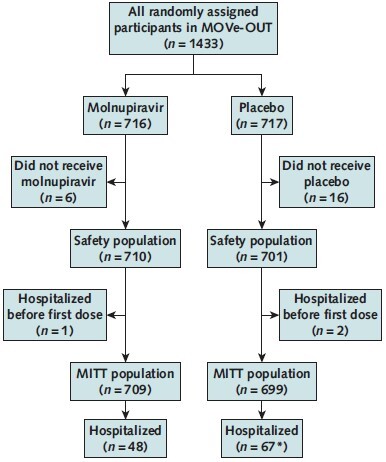
Design: Secondary analysis of the randomized, double-blind, placebo-controlled phase 3 component of MOVe-OUT. (ClinicalTrials.gov: NCT04575597).
Setting: 107 sites globally.
Participants: 1433 nonhospitalized adults aged 18 years or older with mild to moderate COVID-19.
Intervention: Molnupiravir, 800 mg, or placebo every 12 hours for 5 days.
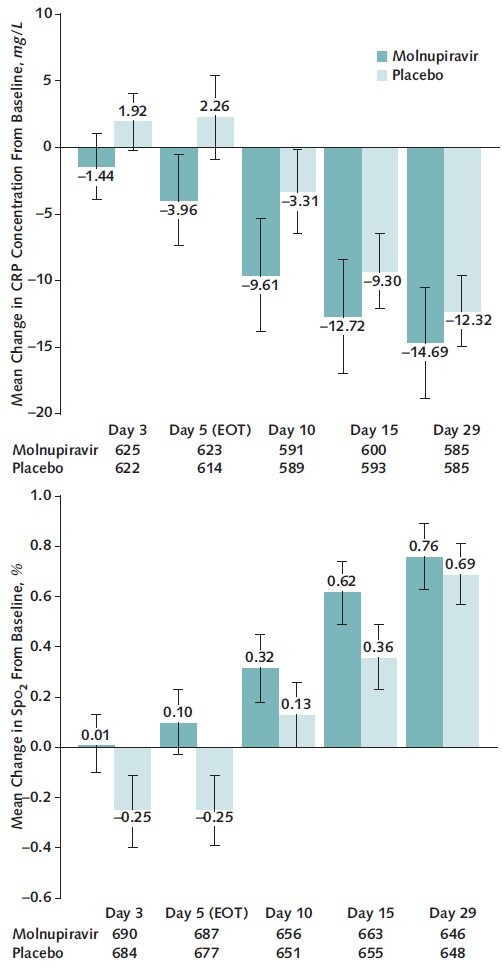
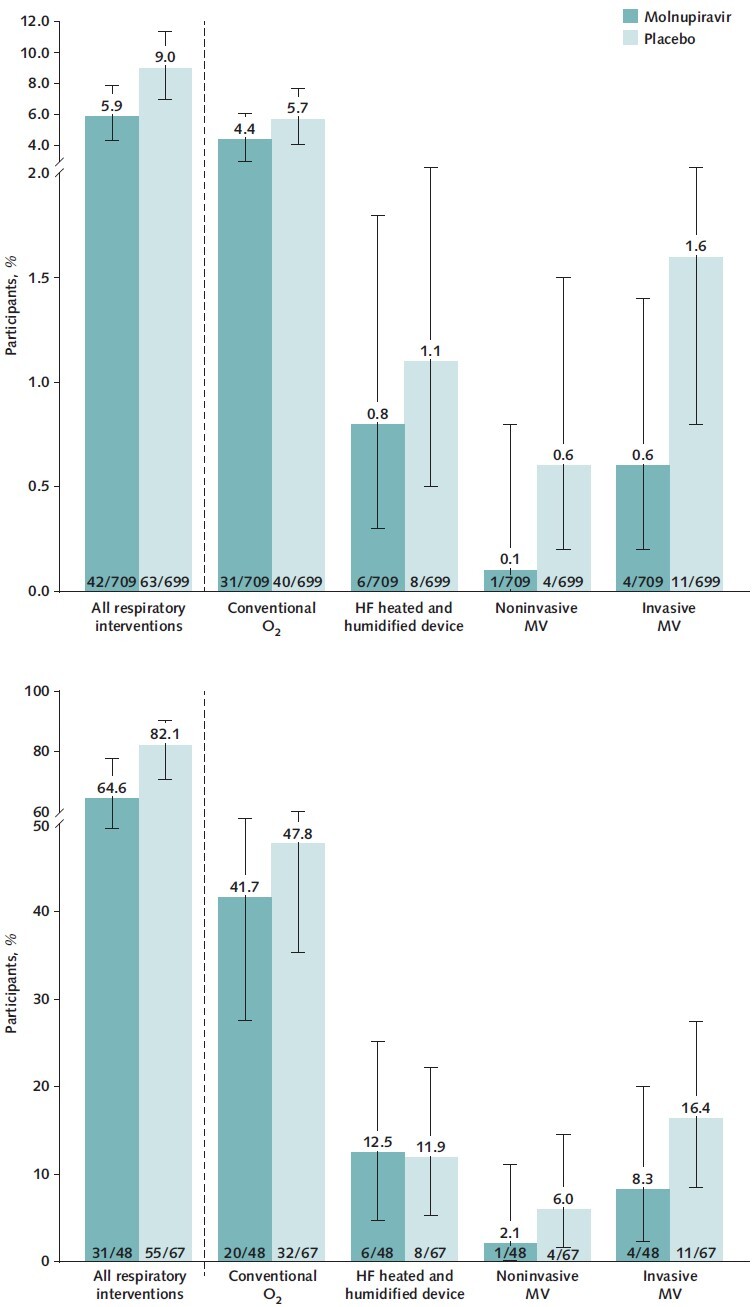
Measurements: Changes from baseline in C-reactive protein (CRP) concentration and oxygen saturation (Spo 2), need for respiratory interventions (including invasive mechanical ventilation), and need for medical services in all randomly assigned participants through day 29, and need for respiratory interventions and time to discharge in the subgroup of participants who were hospitalized after randomization.
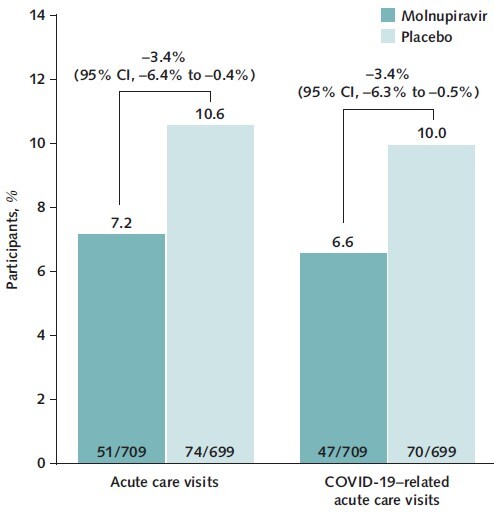
Results: Participants receiving molnupiravir showed faster normalization of CRP and Spo 2, with improvements observed on day 3 of therapy, compared with placebo. Molnupiravir-treated participants had a decreased need for respiratory interventions versus placebo-treated participants (relative risk reduction [RRR], 34.3% [95% CI, 4.3% to 54.9%]), with similar findings in participants who were hospitalized after randomization (RRR, 21.3% [CI, 0.2% to 38.0%]). Hospitalized participants who received molnupiravir were discharged a median of 3 days before those who received placebo. Acute care visits (7.2% vs. 10.6%; RRR, 32.1% [CI, 4.4% to 51.7%]) and COVID-19-related acute care visits (6.6% vs. 10.0%; RRR, 33.8% [CI, 5.6% to 53.6%]) were less frequent in molnupiravir- versus placebo-treated participants.
Limitations: Some analyses were performed post hoc. Longer-term benefits of molnupiravir therapy were not evaluated. Participants were not immunized against SARS-CoV-2.
Conclusion: The findings suggest there are additional important clinical benefits of molnupiravir beyond reduction in hospitalization or death.
Primary funding source: Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc.
Conflict of interest statement
Figures
References
-
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Accessed at https://covid19.who.int on 31 May 2022.
-
- National Institutes of Health. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. 2022. Accessed at www.covid19treatmentguidelines.nih.gov on 17 February 2022. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous