

Immunomodulatory strategies for bone regeneration: A review from the perspective of disease types
- PMID: 35667249
- PMCID: PMC9881498
- DOI: 10.1016/j.biomaterials.2022.121604
Immunomodulatory strategies for bone regeneration: A review from the perspective of disease types
Abstract
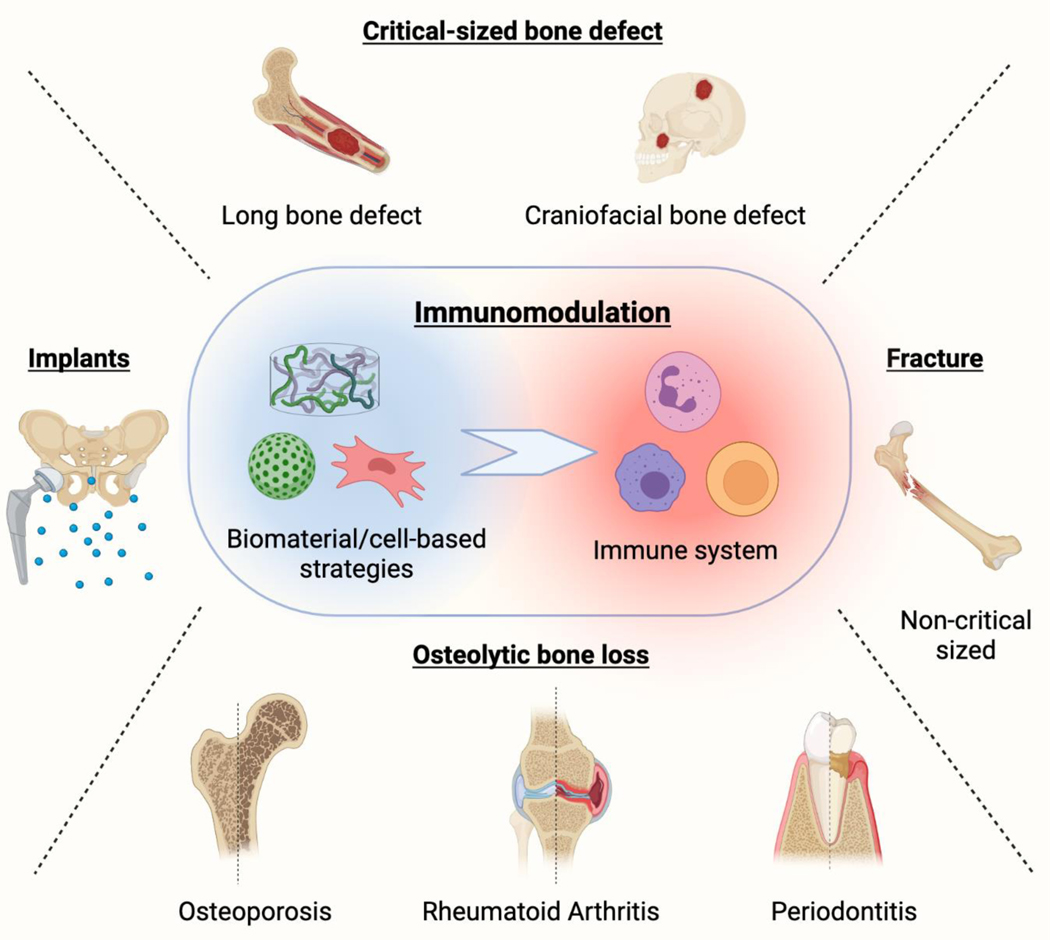
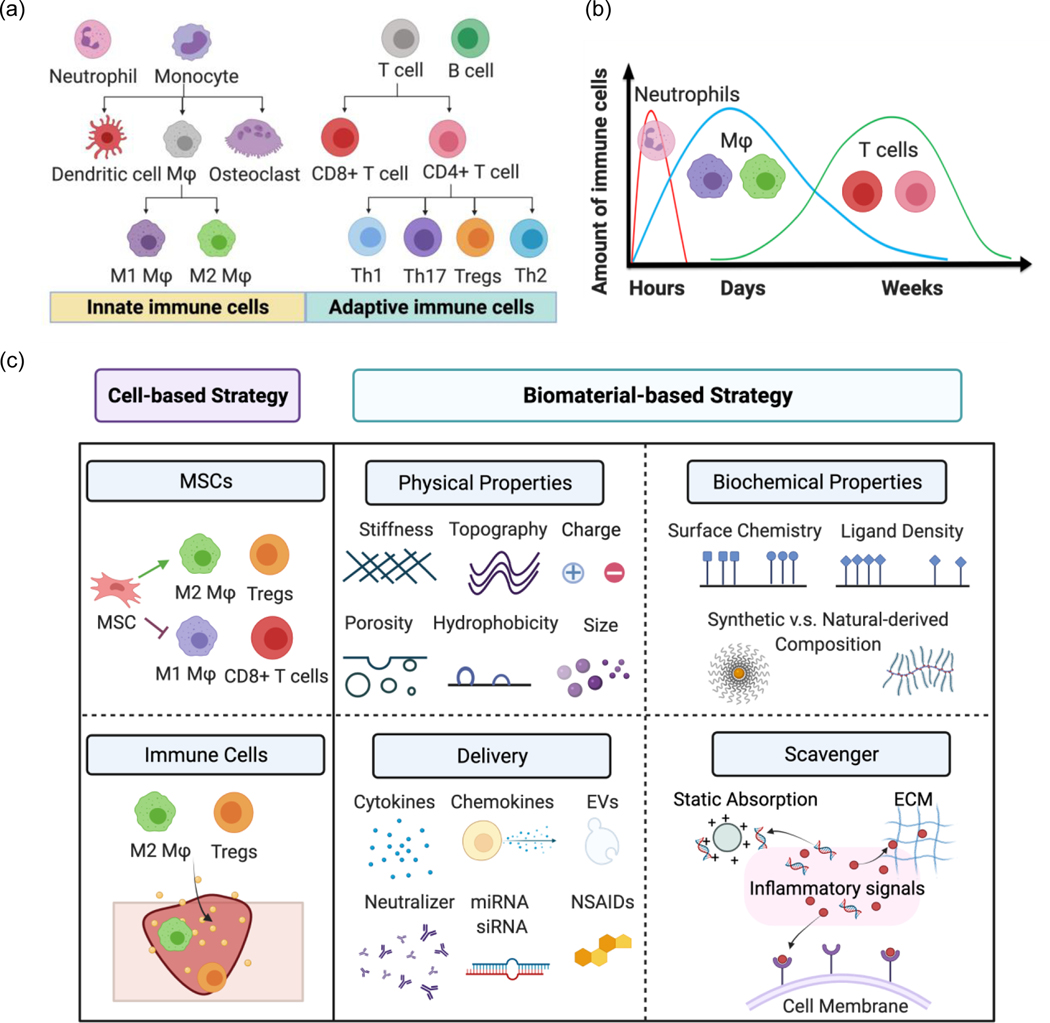
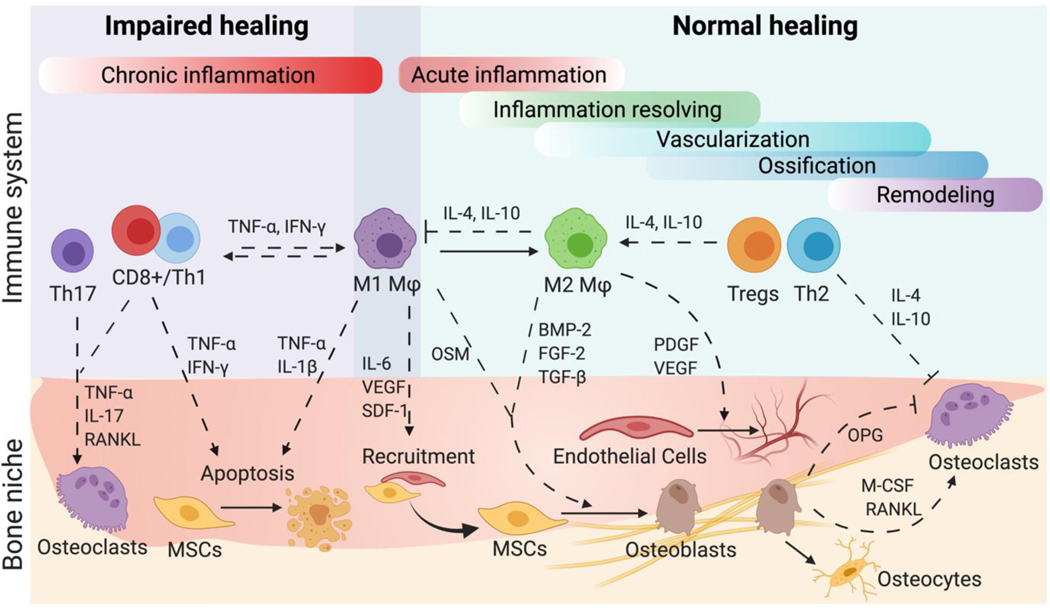
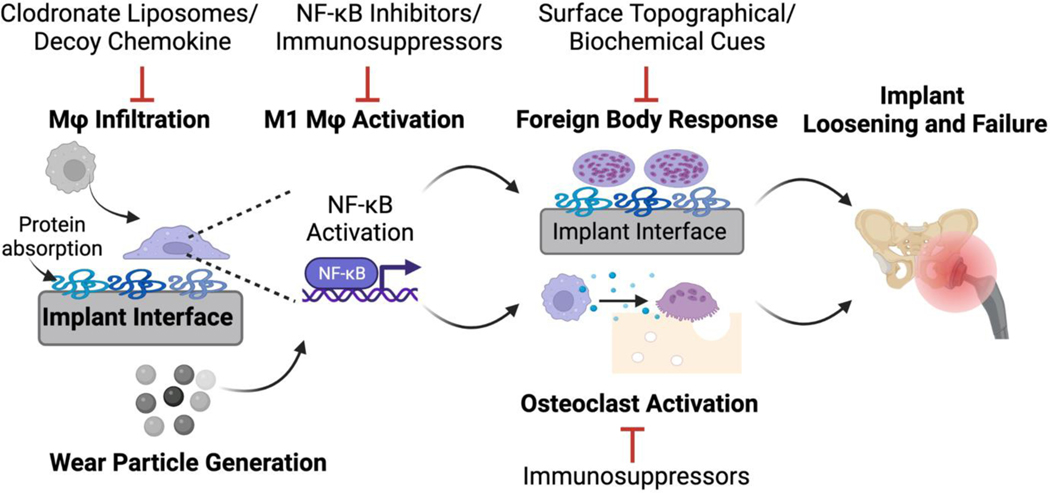
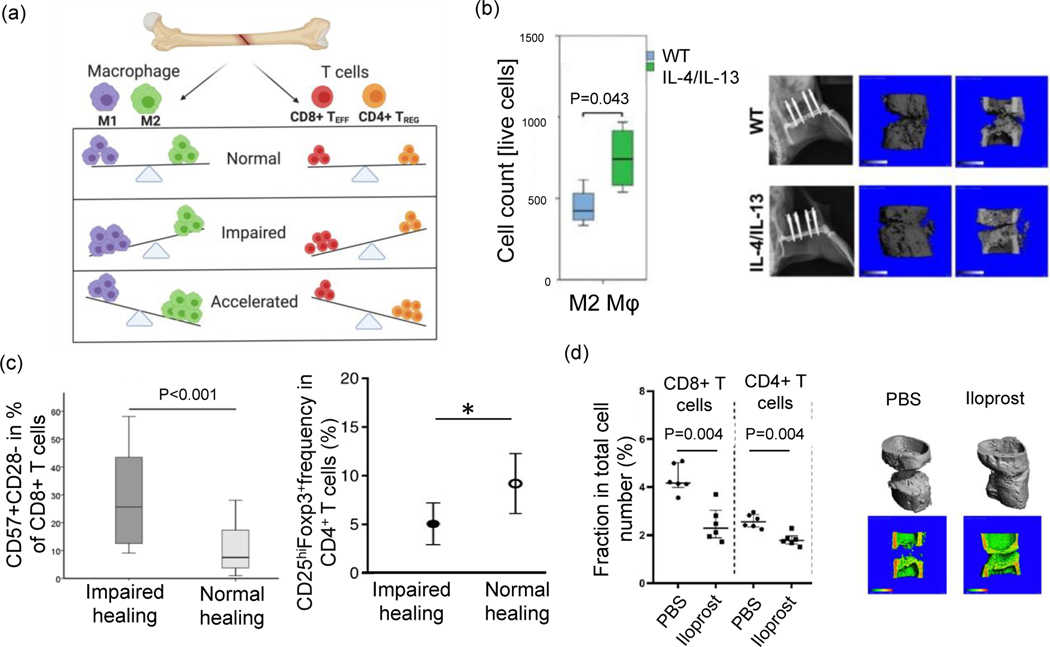
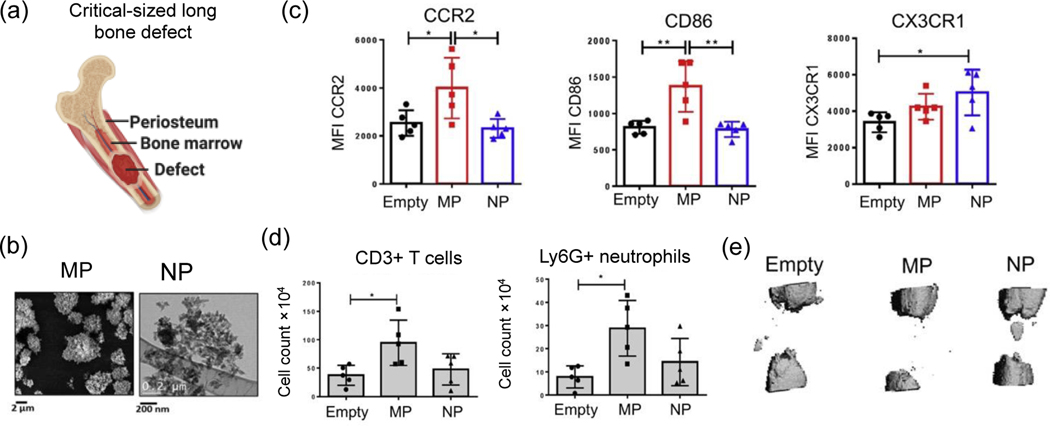
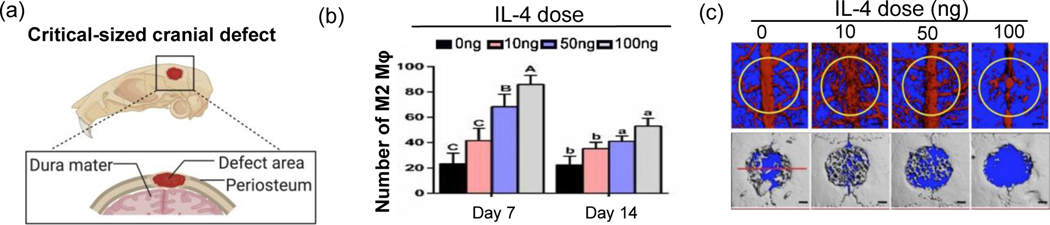
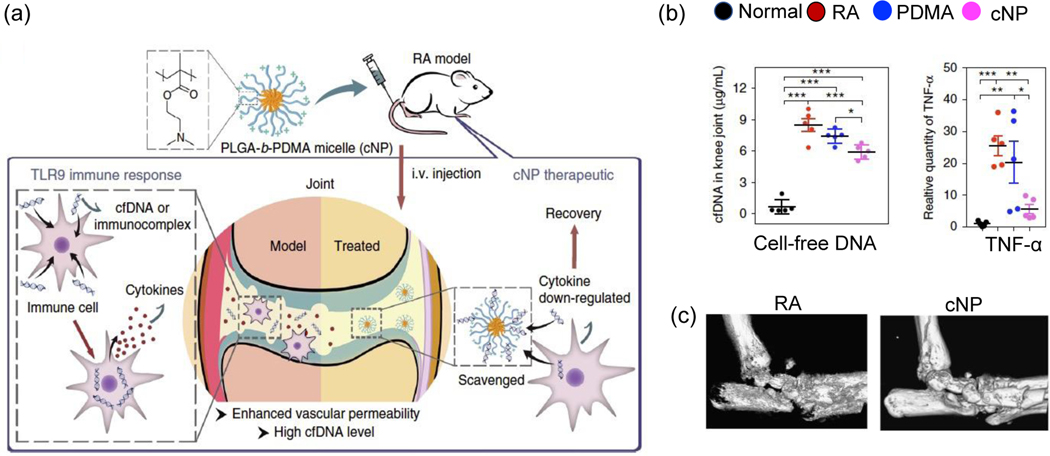
Tissue engineering strategies for treating bone loss to date have largely focused on targeting stem cells or vascularization. Immune cells, including macrophages and T cells, can also indirectly enhance bone healing via cytokine secretion to interact with other bone niche cells. Bone niche cues and local immune environment vary depending on anatomical location, size of defects and disease types. As such, it is critical to evaluate the role of the immune system in the context of specific bone niche and different disease types. This review focuses on immunomodulation research for bone applications using biomaterials and cell-based strategies, with a unique perspective from different disease types. We first reviewed applications for prolonging orthopaedic implant lifetime and enhancing fracture healing, two clinical challenges where immunomodulatory strategies were initially developed for orthopedic applications. We then reviewed recent research progress in harnessing immunomodulatory strategies for regenerating critical-sized, long bone or cranial bone defects, and treating osteolytic bone diseases. Remaining gaps in knowledge, future directions and opportunities were also discussed.
Keywords: Biomaterials; Bone regeneration; Diseases; Immunomodulation.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Figures
References
-
- Yin S, Zhang W, Zhang Z, Jiang X, Recent Advances in Scaffold Design and Material for Vascularized Tissue-Engineered Bone Regeneration, Adv Healthc Mater 8(10) (2019) e1801433. - PubMed
-
- Haggerty AE, Maldonado-Lasunción I, Oudega M, Biomaterials for revascularization and immunomodulation after spinal cord injury, Biomed Mater 13(4) (2018) 044105. - PubMed
-
- Heydari P, Kharaziha M, Varshosaz J, Javanmard SH, Current knowledge of immunomodulation strategies for chronic skin wound repair, J Biomed Mater Res B Appl Biomater 110(2) (2022) 265–288. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
