

A Cost-Utility Analysis of Remote Pulse-Oximetry Monitoring of Patients With COVID-19
- PMID: 35667779
- PMCID: PMC8536499
- DOI: 10.1016/j.jval.2021.09.008
A Cost-Utility Analysis of Remote Pulse-Oximetry Monitoring of Patients With COVID-19
Abstract
Objectives: Since 2020, COVID-19 has infected tens of millions and caused hundreds of thousands of fatalities in the United States. Infection waves lead to increased emergency department utilization and critical care admission for patients with respiratory distress. Although many individuals develop symptoms necessitating a ventilator, some patients with COVID-19 can remain at home to mitigate hospital overcrowding. Remote pulse-oximetry (pulse-ox) monitoring of moderately ill patients with COVID-19 can be used to monitor symptom escalation and trigger hospital visits, as needed.
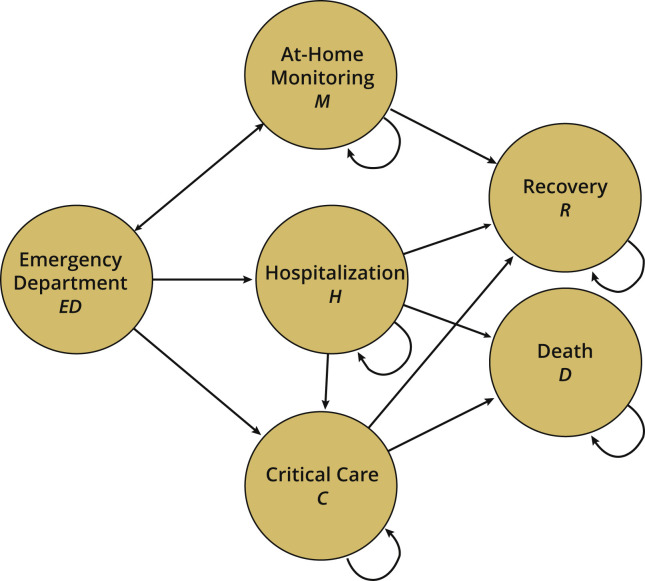
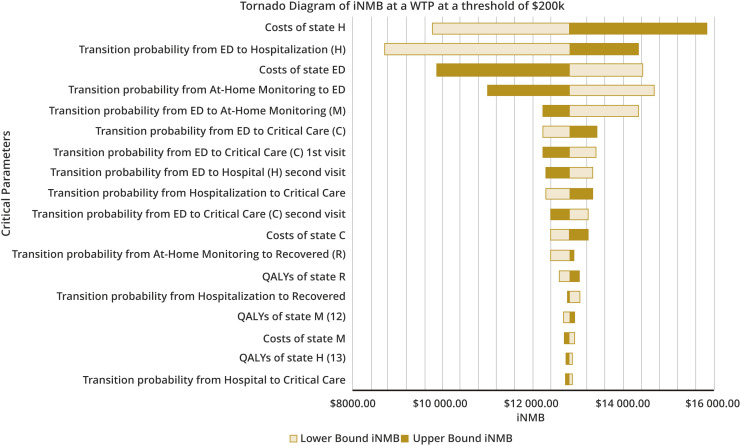
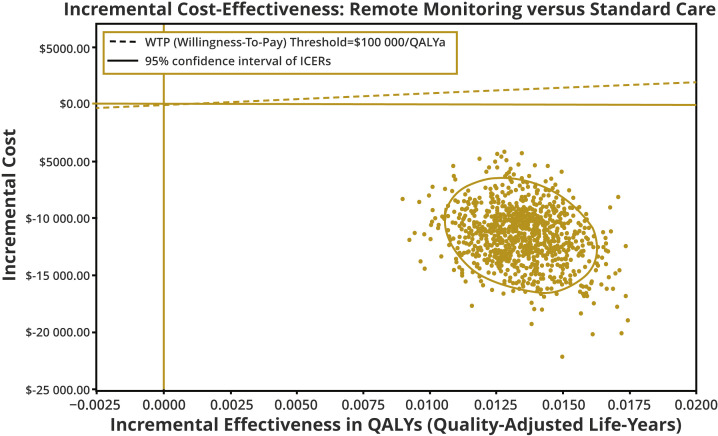
Methods: We analyzed the cost-utility of remote pulse-ox monitoring using a Markov model with a 3-week time horizon and daily cycles from a US health sector perspective. Costs (US dollar 2020) and outcomes were derived from the University Hospitals' real-world evidence and published literature. Costs and quality-adjusted life-years (QALYs) were used to determine the incremental cost-effectiveness ratio at a cost-effectiveness threshold of $100 000 per QALY. We assessed model uncertainty using univariate and probabilistic sensitivity analyses.
Results: Model results demonstrated that remote monitoring dominates current standard care, by reducing costs ($11 472 saved) and improving outcomes (0.013 QALYs gained). There were 87% fewer hospitalizations and 77% fewer deaths among patients with access to remote pulse-ox monitoring. The incremental cost-effectiveness ratio was not sensitive to uncertainty ranges in the model.
Conclusions: Patient with COVID-19 remote pulse-ox monitoring increases the specificity of those requiring follow-up care for escalating symptoms. We recommend remote monitoring adoption across health systems to economically manage COVID-19 volume surges, maintain patients' comfort, reduce community infection spread, and carefully monitor needs of multiple individuals from one location by trained experts.
Keywords: COVID-19; critical care; emergency department; infectious disease; intensive care unit; pulse oximetry; telemedicine.
Copyright © 2021 International Society for Pharmacoeconomics and Outcomes Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- COVID-19 map Baltimore: Johns Hopkins Coronavirus Resource Center. https://coronavirus.jhu.edu/
-
- Tracking COVID-19 in CA. California State Government. https://covid19.ca.gov/
-
- HHS protect public data hub: state representative estimates for hospital utilization. US Department of Health and Human Services. https://protect-public.hhs.gov/
-
- Murthy S., Gomersall C.D., Fowler R.A. Care for critically ill patients with COVID-19. JAMA. 2020;323(15):1499–1500. - PubMed
-
- 2020 AHA hospital statistics. American Hospital Association. https://www.aha.org/system/files/media/file/2020/01/2020-aha-hospital-fa...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
