

Observational study of population genomic screening for variants associated with endocrine tumor syndromes in a large, healthcare-based cohort
- PMID: 35668420
- PMCID: PMC9172012
- DOI: 10.1186/s12916-022-02375-4
Observational study of population genomic screening for variants associated with endocrine tumor syndromes in a large, healthcare-based cohort
Abstract
Background: In current care, patients' personal and self-reported family histories are primarily used to determine whether genetic testing for hereditary endocrine tumor syndromes (ETS) is indicated. Population genomic screening for other conditions has increased ascertainment of individuals with pathogenic/likely pathogenic (P/LP) variants, leading to improved management and earlier diagnoses. It is unknown whether such benefits occur when screening broader populations for P/LP ETS variants. This manuscript assesses clinical utility outcomes of a large, unselected, healthcare-based genomic screening program by describing personal and family history of syndrome-related features, risk management behaviors after result disclosure, and rates of relevant post-disclosure diagnoses in patient-participants with P/LP ETS variants.
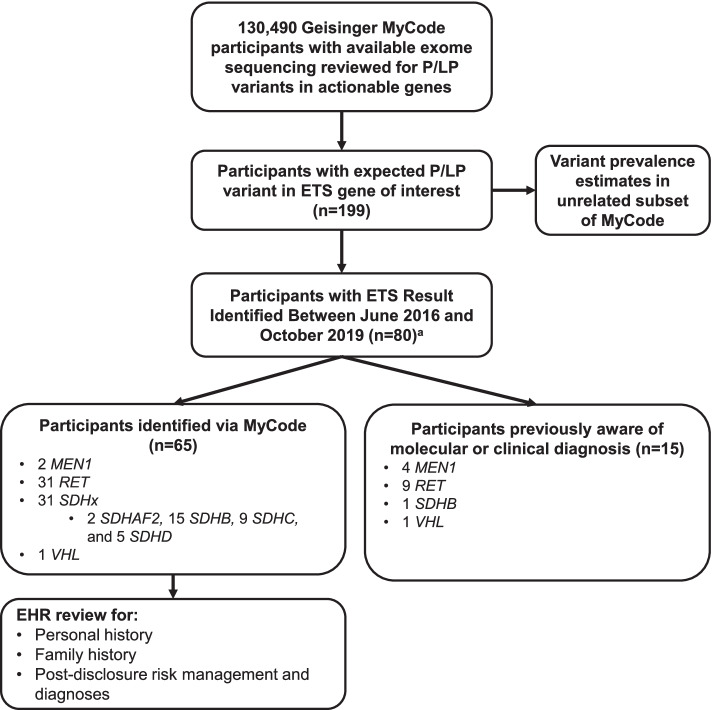
Methods: Observational study of individuals informed of a P/LP variant in MEN1, RET, SDHAF2, SDHB, SDHC, SDHD, or VHL through Geisinger's MyCode Community Health Initiative between June 2016 and October 2019. Electronic health records (EHRs) of participants were evaluated for a report of pre-disclosure personal and self-reported family histories and post-disclosure risk management and diagnoses.
Results: P/LP variants in genes of interest were identified in 199 of 130,490 (1 in 656) adult Geisinger MyCode patient-participants, 80 of which were disclosed during the study period. Eighty-one percent (n = 65) did not have prior evidence of the result in their EHR and, because they were identified via MyCode, were included in further analyses. Five participants identified via MyCode (8%) had a personal history of syndrome-related features; 16 (25%) had a positive self-reported family history. Time from result disclosure to EHR review was a median of 0.7 years. Post-disclosure, 36 (55.4%) completed a recommended risk management behavior; 11 (17%) were diagnosed with a syndrome-related neoplasm after completing a risk management intervention.
Conclusions: Broader screening for pathogenic/likely pathogenic variants associated with endocrine tumor syndromes enables detection of at-risk individuals, leads to the uptake of risk management, and facilitates relevant diagnoses. Further research will be necessary to continue to determine the clinical utility of screening diverse, unselected populations for such variants.
Keywords: Genomic screening; MEN 1; MEN 2; Medullary thyroid cancer; Paraganglioma; Succinate dehydrogenase; VHL.
© 2022. The Author(s).
Conflict of interest statement
JMS, NMO, GMT, WSM, MAK, AB1, MLGH, JM, NCP, MMA, and MSW have nothing to declare. ACS receives grant funding (8/20/2019-7/31/2024) from the NIH All of Us Research Program’s Genetic Counseling Resource in her role as Chair to the Genetic Counseling Resource Advisory Board. AB2 receives compensation as an editorial board member for the
Figures
References
-
- McKusick-Nathans Institute of Genetic Medicine, Johns Hopkins University. [cited November 19, 2021]. Available from: https://omim.org/.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
