

Respiratory distress observation scales to predict weaning outcome
- PMID: 35668459
- PMCID: PMC9169318
- DOI: 10.1186/s13054-022-04028-7
Respiratory distress observation scales to predict weaning outcome
Abstract
Background: Whether dyspnea is present before starting a spontaneous breathing trial (SBT) and whether it may affect the outcome of the SBT is unknown. Mechanical Ventilation-Respiratory Distress Observation Scale (MV-RDOS) has been proposed as a reliable surrogate of dyspnea in non-communicative intubated patients. In the present study, we sought (1) to describe the evolution of the MV-RDOS during a SBT and (2) to investigate whether MV-RDOS can predict the outcome of the SBT.
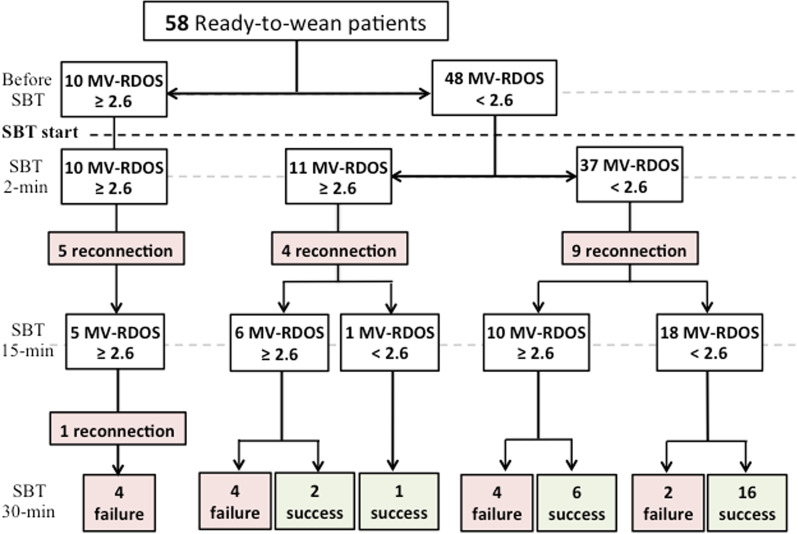
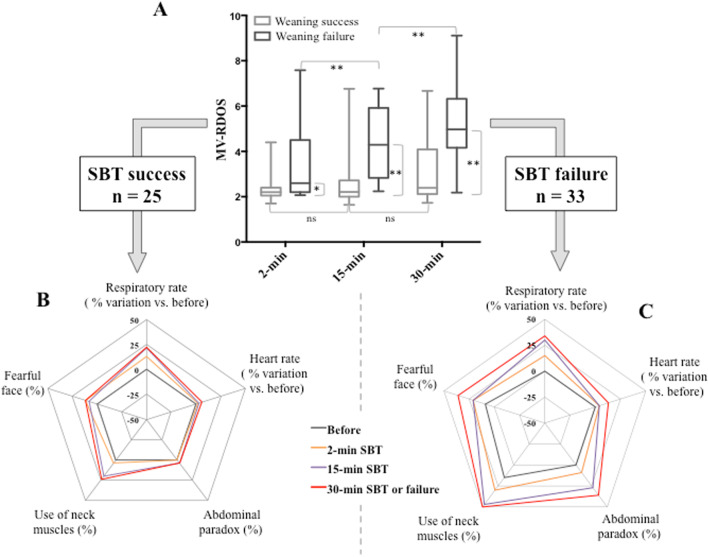
Methods: Prospective, single-center study in a twenty-two bed ICU in a tertiary center. Patients intubated since more 48 h who had failed a first SBT were eligible if they meet classical readiness to wean criteria. The MV-RDOS was assessed before, at 2-min, 15-min and 30-min (end) of the SBT. The presence of clinically important dyspnea was inferred by a MV-RDOS value ≥ 2.6.
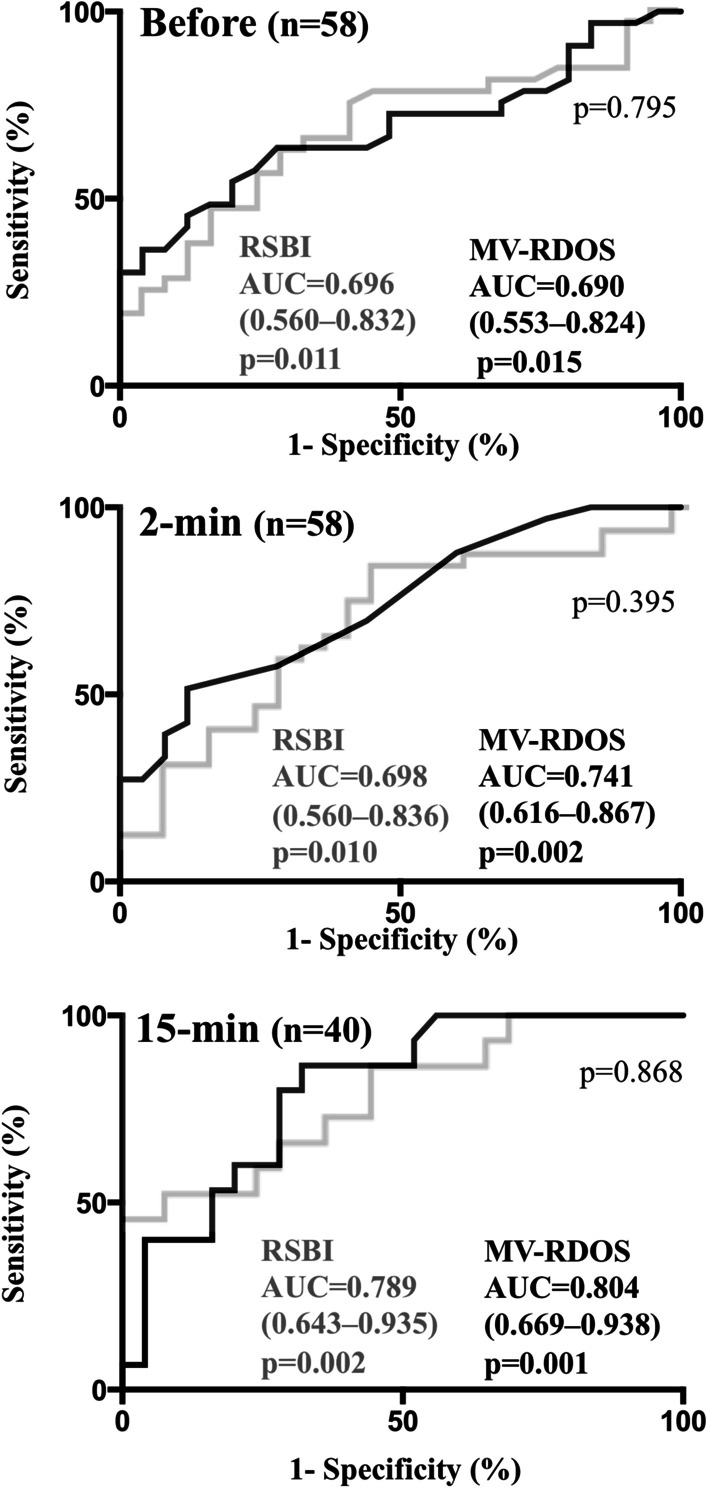
Results: Fifty-eight patients (age 63 [51-70], SAPS II 66 [51-76]; med [IQR]) were included. Thirty-three (57%) patients failed the SBT, whose 18 (55%) failed before 15-min. Twenty-five (43%) patients successfully passed the SBT. A MV-RDOS ≥ 2.6 was present in ten (17%) patients before to start the SBT. All these ten patients subsequently failed the SBT. A MV-RDOS ≥ 2.6 at 2-min predicted a SBT failure with a 51% sensibility and a 88% specificity (AUC 0.741 95% confidence interval [CI] 0.616-0.866, p = 0.002). Best cut-off value at 2-min was 4.3 and predicted SBT failure with a 27% sensibility and a 96% specificity.
Conclusion: Despite patients met classical readiness to wean criteria, respiratory distress assessed with the MV-RDOS was frequent at the beginning of SBT. Measuring MV-RDOS before to initiate a SBT could avoid undue procedure and reduce patient's exposure to unnecessary mechanical ventilation weaning failure and distress.
Keywords: Critical care; Dyspnea; Dyspnea observation scale; Intensive care unit; Respiratory Distress Observation Scale; Spontaneous breathing trial; Weaning from mechanical ventilation.
© 2022. The Author(s).
Conflict of interest statement
Maxens Decavèle reports personal fees (for congress registration) from ISIS Medical. Thomas Similowski reports personal fees from AstraZeneca France, personal fees from Boerhinger Ingelheim France, personal fees and non-financial support from Novartis France, personal fees from TEVA France, personal fees from Chiesi France, personal fees from Lungpacer Inc, personal fees from ADEP Assistance, grants from Air Liquide Medical Systems, outside the submitted work. Alexandre Demoule reports grants, personal fees and non-financial support from Philips, personal fees from Baxter, personal fees and non-financial support from Fisher & Paykel, grants from French Ministry of Health, personal fees from Getinge, grants, personal fees and non-financial support from Respinor, grants, personal fees and non-financial support from Lungpacer, personal fees from Lowenstein, personal fees from Gilead, outside the submitted work. Martin Dres reports expertise fees, travel expenses, research contract from Lungpacer, research contract from Bioserenity, and congress registration fees from Dräger, outside the submitted work. Capucine Morélot-Panzini reports personal fees from Astra-Zeneca, GSK, SOS Oxygène, ADEP, ISIS, Resmed, Chiesi, Menarini, Vivisol, Air Liquide, Lowenstein, Fisher & Paykel, outside the submitted work. Julien Mayaux reports personal fees (for congress registration) from Gilead France. Emmanuel Rozenberg, Elise Morawiec and Marie-Cécile Niérat, have no conflicts of interests to declare.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
