

Alloimmune Risk Stratification for Kidney Transplant Rejection
- PMID: 35669972
- PMCID: PMC9163827
- DOI: 10.3389/ti.2022.10138
Alloimmune Risk Stratification for Kidney Transplant Rejection
Abstract
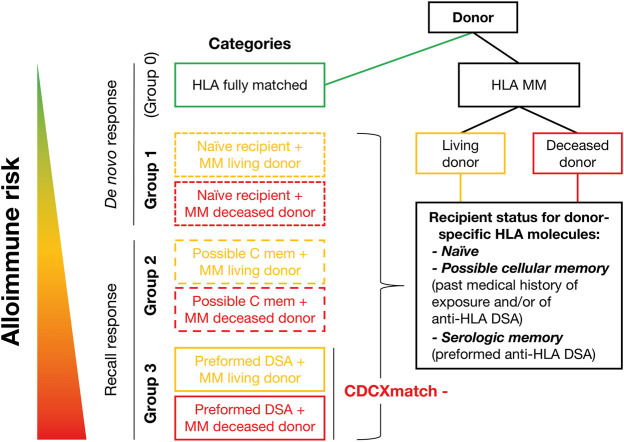
Different types of kidney transplantations are performed worldwide, including biologically diverse donor/recipient combinations, which entail distinct patient/graft outcomes. Thus, proper immunological and non-immunological risk stratification should be considered, especially for patients included in interventional randomized clinical trials. This paper was prepared by a working group within the European Society for Organ Transplantation, which submitted a Broad Scientific Advice request to the European Medicines Agency (EMA) relating to clinical trial endpoints in kidney transplantation. After collaborative interactions, the EMA sent its final response in December 2020, highlighting the following: 1) transplantations performed between human leukocyte antigen (HLA)-identical donors and recipients carry significantly lower immunological risk than those from HLA-mismatched donors; 2) for the same allogeneic molecular HLA mismatch load, kidney grafts from living donors carry significantly lower immunological risk because they are better preserved and therefore less immunogenic than grafts from deceased donors; 3) single-antigen bead testing is the gold standard to establish the repertoire of serological sensitization and is used to define the presence of a recipient's circulating donor-specific antibodies (HLA-DSA); 4) molecular HLA mismatch analysis should help to further improve organ allocation compatibility and stratify immunological risk for primary alloimmune activation, but without consensus regarding which algorithm and cut-off to use it is difficult to integrate information into clinical practice/study design; 5) further clinical validation of other immune assays, such as those measuring anti-donor cellular memory (T/B cell ELISpot assays) and non-HLA-DSA, is needed; 6) routine clinical tests that reliably measure innate immune alloreactivity are lacking.
Keywords: alloimmune risk; crossmatch; high-risk transplantation; individualized immunosuppression; molecular HLA mismatch.
Copyright © 2022 Bestard, Thaunat, Bellini, Böhmig, Budde, Claas, Couzi, Furian, Heemann, Mamode, Oberbauer, Pengel, Schneeberger and Naesens.
Conflict of interest statement
OB has received research funding from Chiesi and served as adviser for Hansa Biopharma. OT has received research funding from bioMérieux, Bristol Myers Squibb, and Immucor; and has consultancy agreements with Biotest and Novartis. GB has received honoraria and/or research funding from Astellas, CareDx, CSL Behring, Fresenius, Hansa, Neovii, and Vitaeris. KB has received honoraria and/or research funding from Alexion, Astellas, Bristol Myers Squibb, Chiesi, Fresenius, Hansa, Hexal, Merck, Novartis, Otsuka, Pfizer, Roche, Sandoz, Siemens, and Veloxis. FC is a scientific adviser for GenDx and Immucor. LF has received honoraria and/or research funding from Astellas, Chiesi, Hansa, and Novartis. UH has received grants/research support from Baxter, Chiesi, and Neovii; speakers’ bureaux/honoraria from Chiesi and Hansa; and consulting fees from Astellas, Hansa, Neovii, Novartis, and Teva. NM has received honoraria from Hansa, Chiesi, Novartis, and Takeda. RO has received grants/research support from Amgen, Astellas, and Chiesi; and speakers’ bureaux/honoraria from Amgen, Astellas, Chiesi, Hansa, Neovii, Novartis, and Teva. SS has received grants/research support from Bridge to Life, Chiesi, Neovii, Novartis, Organ Recovery Systems, and Sandoz; speakers’ bureaux/honoraria from Astellas, BMS, Chiesi, Novartis, OrganOx, and Sanofi; and consulting fees from Astellas, Atara, Merck, NefroHealth, Novartis, Sandoz, and Teva. The remaining authors declare that the work was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Eurotransplant. Statistics. Available from: https://www.eurotransplant.org/statistics/statistics-library/ (Accessed January 15, 2021).
-
- Süsal C, Wettstein D, Döhler B, MorathRuhenstroth CA, Ruhenstroth A, Scherer S, et al. Association of Kidney Graft Loss with De Novo Produced Donor-specific and Non-donor-specific HLA Antibodies Detected by Single Antigen Testing. Transplantation (2015) 99:1976–80. 10.1097/tp.0000000000000672 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials