

Partition of respiratory mechanics in patients with acute respiratory distress syndrome and association with outcome: a multicentre clinical study
- PMID: 35670818
- PMCID: PMC9171739
- DOI: 10.1007/s00134-022-06724-y
Partition of respiratory mechanics in patients with acute respiratory distress syndrome and association with outcome: a multicentre clinical study
Erratum in
-
Correction: Partition of respiratory mechanics in patients with acute respiratory distress syndrome and association with outcome: a multicentre clinical study.Intensive Care Med. 2023 Mar;49(3):386. doi: 10.1007/s00134-023-06985-1. Intensive Care Med. 2023. PMID: 36729185 Free PMC article. No abstract available.
Abstract
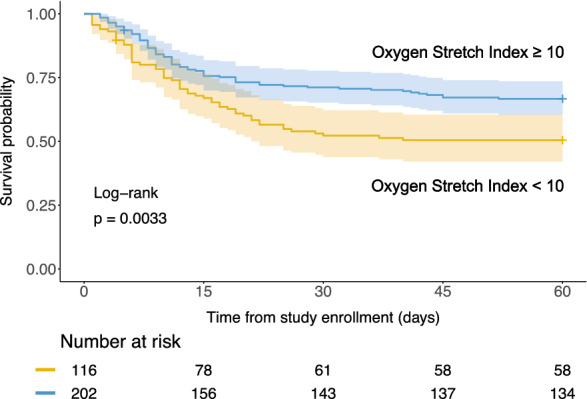
Purpose: In acute respiratory distress syndrome (ARDS), physiological parameters associated with outcome may help defining targets for mechanical ventilation. This study aimed to address whether transpulmonary pressures (PL), including transpulmonary driving pressure (DPL), elastance-derived plateau PL, and directly-measured end-expiratory PL, are better associated with 60-day outcome than airway driving pressure (DPaw). We also tested the combination of oxygenation and stretch index [PaO2/(FiO2*DPaw)].
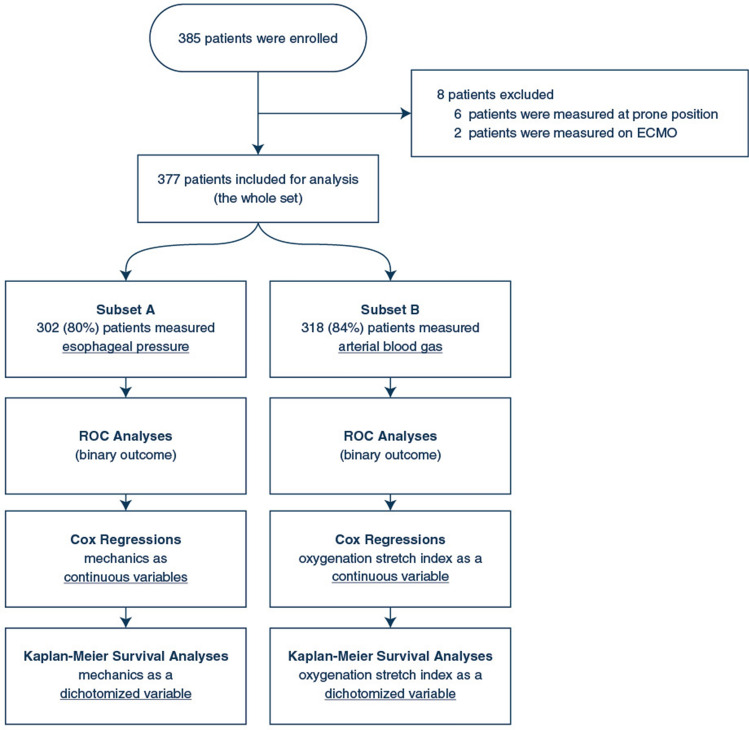
Methods: Prospective, observational, multicentre registry of ARDS patients. Respiratory mechanics were measured early after intubation at 6 kg/ml tidal volume. We compared the predictive power of the parameters for mortality at day-60 through receiver operating characteristic (ROC) and assessed their association with 60-day mortality through unadjusted and adjusted Cox regressions. Finally, each parameter was dichotomized, and Kaplan-Meier survival curves were compared.
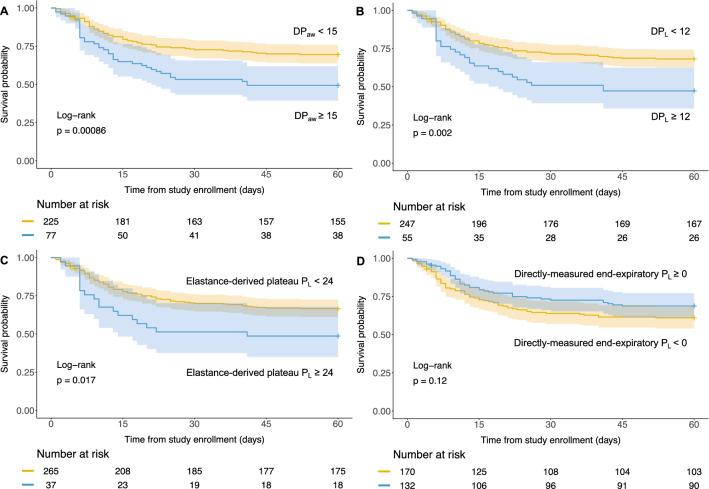
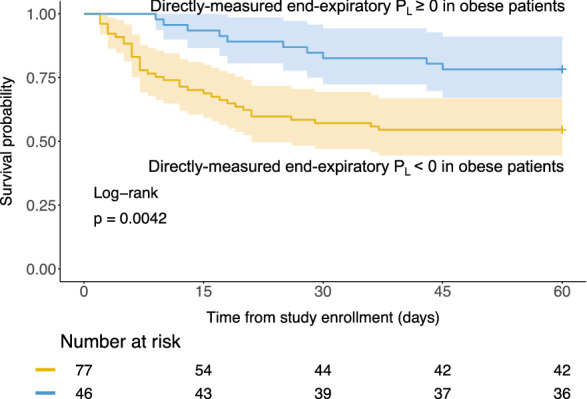
Results: 385 patients were enrolled 2 [1-4] days from intubation (esophageal pressure and arterial blood gases in 302 and 318 patients). As continuous variables, DPaw, DPL, and oxygenation stretch index were associated with 60-day mortality after adjustment for age and Sequential Organ Failure Assessment, whereas elastance-derived plateau PL was not. DPaw and DPL performed equally in ROC analysis (P = 0.0835). DPaw had the best-fit Cox regression model. When dichotomizing the variables, DPaw ≥ 15, DPL ≥ 12, plateau PL ≥ 24, and oxygenation stretch index < 10 exhibited lower 60-day survival probability. Directly measured end-expiratory PL ≥ 0 was associated with better outcome in obese patients.
Conclusion: DPL was equivalent predictor of outcome than DPaw. Our study supports the soundness of limiting lung and airway driving pressure and maintaining positive end-expiratory PL in obese patients.
Keywords: Acute respiratory distress syndrome; Artificial respiration; Mechanical ventilation; Positive-pressure respiration; Respiratory mechanics.
© 2022. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
All authors declared having no conflict of interest related to this work. Unrelated potential conflict are as follows: FB received research support from GE Healthcare, Medtronic and Getinge Group, consulting fees from Löwenstein Medical and travel fees from Air Liquide Medical System, which are not related to the present study. LB’s laboratory received research grants from Medtronic and Draeger, equipment from Sentec, Fisher Paykel, Philips and Air Liquide, and lecture fees from Fisher Paykel.
Figures
Comment in
-
Possible overestimation of chest wall driving pressure and underestimation of airway closure.Intensive Care Med. 2023 Feb;49(2):258-259. doi: 10.1007/s00134-022-06945-1. Epub 2022 Dec 16. Intensive Care Med. 2023. PMID: 36525133 Free PMC article. No abstract available.
References
-
- Acute Respiratory Distress Syndrome N. Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. doi: 10.1056/NEJM200005043421801. - DOI - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, Ranieri M, Rubenfeld G, Thompson BT, Wrigge H, Slutsky AS, Pesenti A, Investigators LS, Group ET. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315:788–800. doi: 10.1001/jama.2016.0291. - DOI - PubMed
-
- Urner M, Juni P, Hansen B, Wettstein MS, Ferguson ND, Fan E. Time-varying intensity of mechanical ventilation and mortality in patients with acute respiratory failure: a registry-based, prospective cohort study. Lancet Respir Med. 2020;8:905–913. doi: 10.1016/S2213-2600(20)30325-8. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
