

Epigenetic priming enhances antitumor immunity in platinum-resistant ovarian cancer
- PMID: 35671108
- PMCID: PMC9282926
- DOI: 10.1172/JCI158800
Epigenetic priming enhances antitumor immunity in platinum-resistant ovarian cancer
Abstract
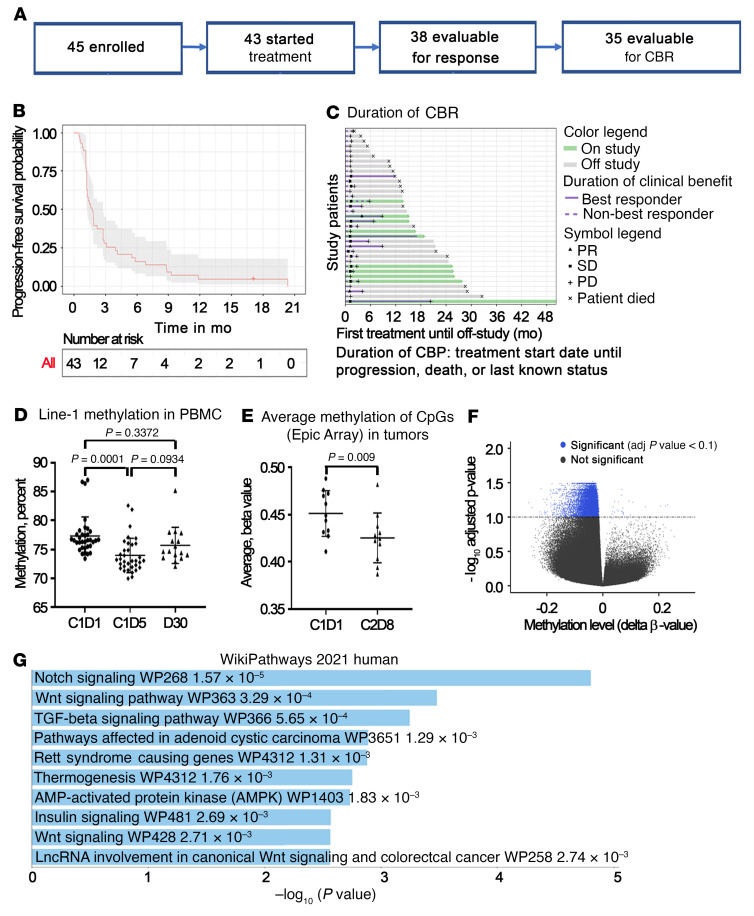
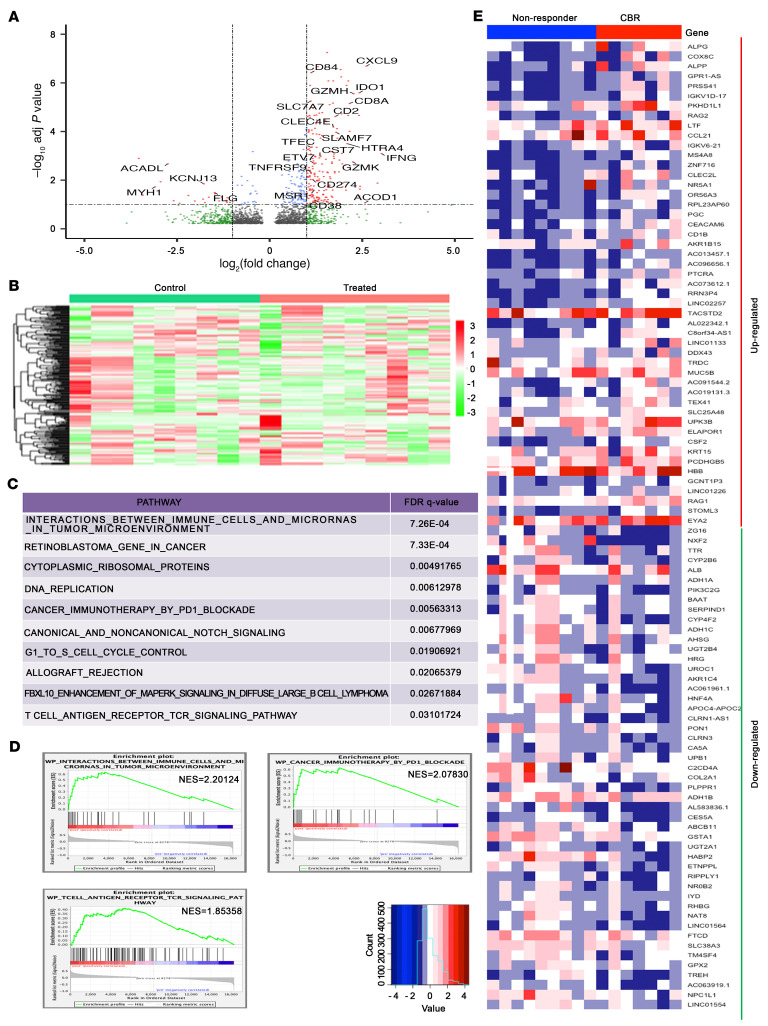
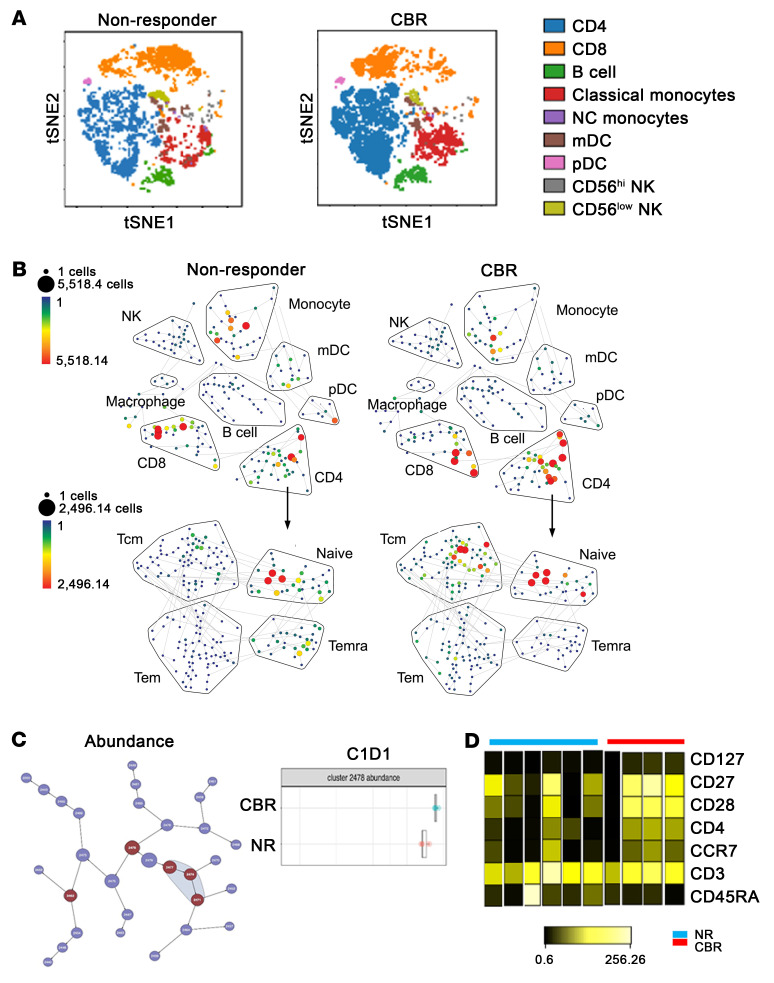
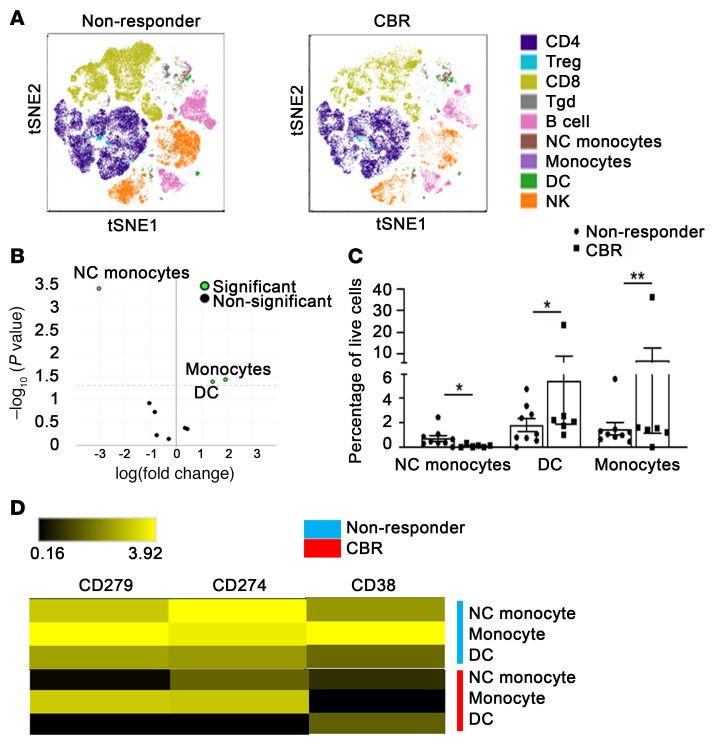
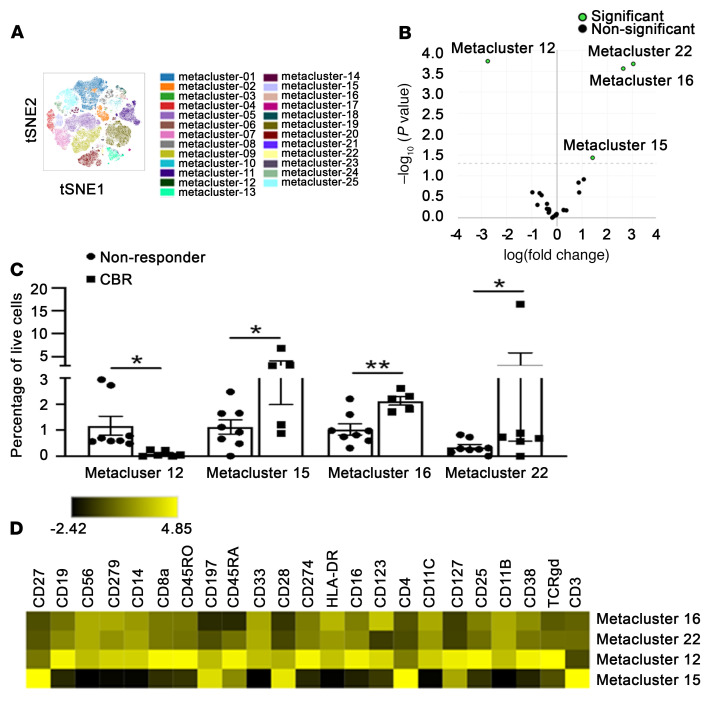
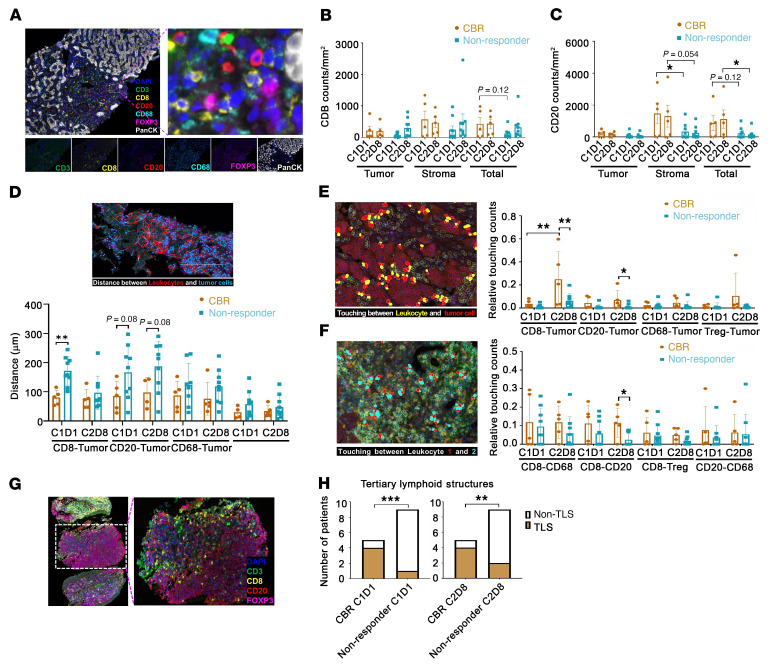
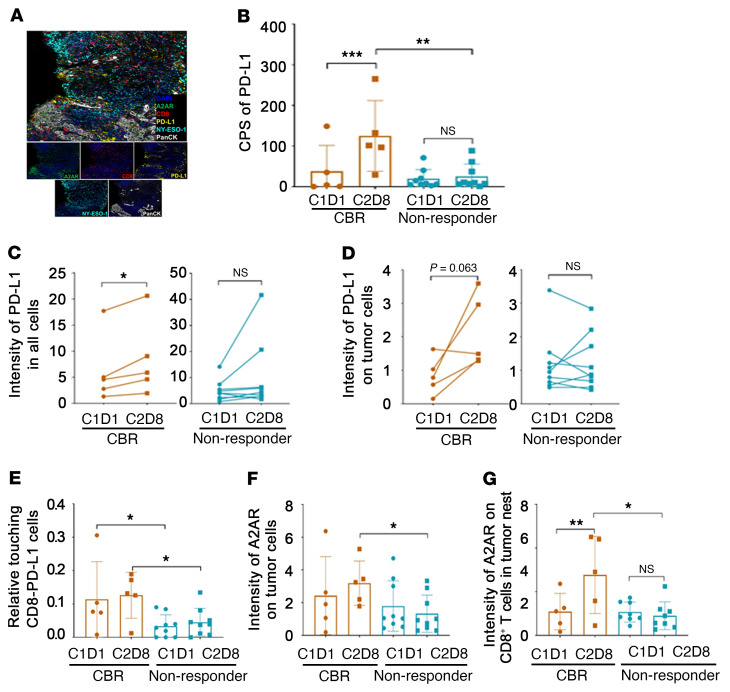
BackgroundImmune checkpoint inhibitors (ICIs) have modest activity in ovarian cancer (OC). To augment their activity, we used priming with the hypomethylating agent guadecitabine in a phase II study.MethodsEligible patients had platinum-resistant OC, normal organ function, measurable disease, and received up to 5 prior regimens. The treatment included guadecitabine (30 mg/m2) on days 1-4, and pembrolizumab (200 mg i.v.) on day 5, every 21 days. The primary endpoint was the response rate. Tumor biopsies, plasma, and PBMCs were obtained at baseline and after treatment.ResultsAmong 35 evaluable patients, 3 patients had partial responses (8.6%), and 8 (22.9%) patients had stable disease, resulting in a clinical benefit rate of 31.4% (95% CI: 16.9%-49.3%). The median duration of clinical benefit was 6.8 months. Long-interspersed element 1 (LINE1) was hypomethylated in post-treatment PBMCs, and methylomic and transcriptomic analyses showed activation of antitumor immunity in post-treatment biopsies. High-dimensional immune profiling of PBMCs showed a higher frequency of naive and/or central memory CD4+ T cells and of classical monocytes in patients with a durable clinical benefit or response (CBR). A higher baseline density of CD8+ T cells and CD20+ B cells and the presence of tertiary lymphoid structures in tumors were associated with a durable CBR.ConclusionEpigenetic priming using a hypomethylating agent with an ICI was feasible and resulted in a durable clinical benefit associated with immune responses in selected patients with recurrent OC.Trial registrationClinicalTrials.gov NCT02901899.FundingUS Army Medical Research and Material Command/Congressionally Directed Medical Research Programs (USAMRMC/CDMRP) grant W81XWH-17-0141; the Diana Princess of Wales Endowed Professorship and LCCTRAC funds from the Robert H. Lurie Comprehensive Cancer Center; Walter S. and Lucienne Driskill Immunotherapy Research funds; Astex Pharmaceuticals; Merck & Co.; National Cancer Institute (NCI), NIH grants CCSG P30 CA060553, CCSG P30 CA060553, and CA060553.
Keywords: Cancer; Cancer immunotherapy; Epigenetics; Immunology; Oncology.
Figures
Comment in
-
Inhibiting DNA methylation improves antitumor immunity in ovarian cancer.J Clin Invest. 2022 Jul 15;132(14):e160186. doi: 10.1172/JCI160186. J Clin Invest. 2022. PMID: 35838045 Free PMC article.
References
-
- Pujade-Lauraine E, et al. Avelumab alone or in combination with chemotherapy versus chemotherapy alone in platinum-resistant or platinum-refractory ovarian cancer (JAVELIN Ovarian 200): an open-label, three-arm, randomised, phase 3 study. Lancet Oncol. 2021;22(7):1034–1046. doi: 10.1016/S1470-2045(21)00216-3. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
