

Effects of Varying Laser Parameters During Laser Stapedotomy on Intracochlear Pressures
- PMID: 35671134
- PMCID: PMC10097413
- DOI: 10.1177/01945998221104658
Effects of Varying Laser Parameters During Laser Stapedotomy on Intracochlear Pressures
Abstract
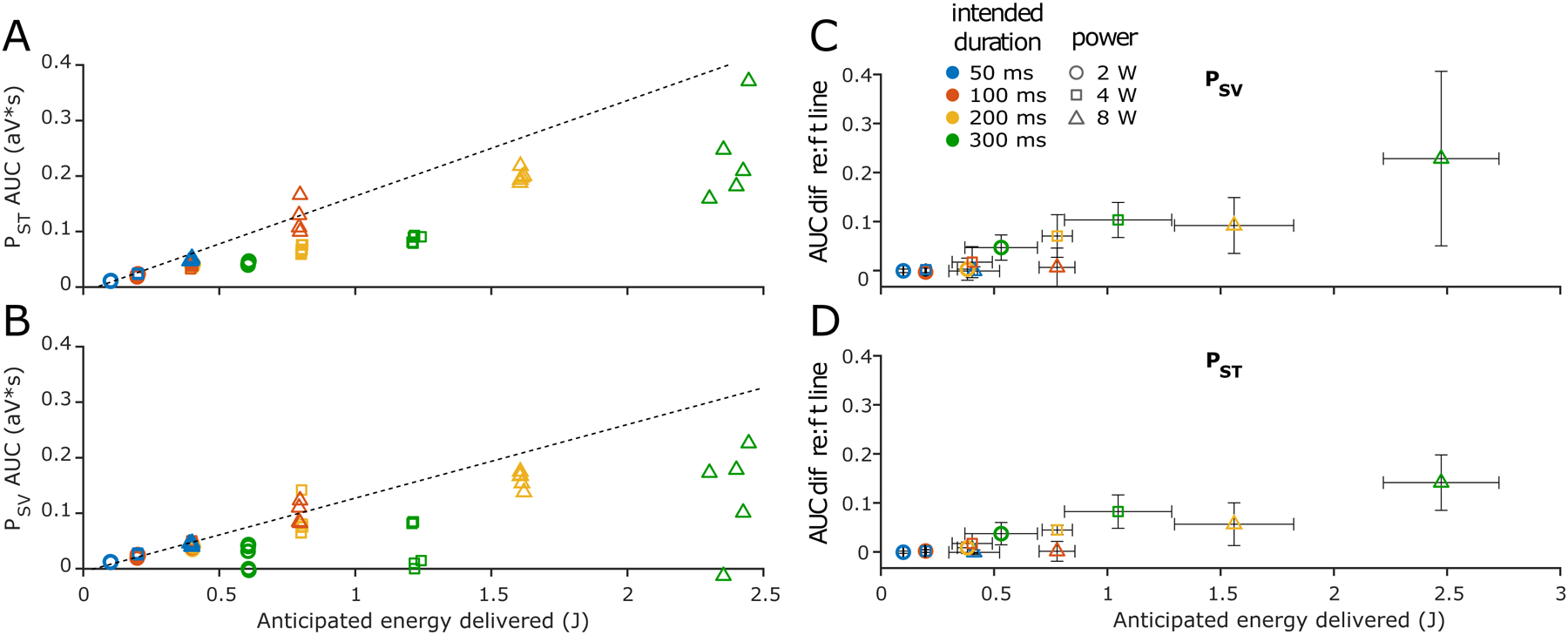
Objective: Sensorineural hearing loss is a known complication of stapes surgery. We previously showed that laser stapedotomy can result in intracochlear pressures that are comparable to high sound pressure levels. Optimizing laser settings to those that correspond with the lowest pressure changes may mitigate risk for postoperative hearing loss. Here we quantify the effects of various laser parameters on intracochlear pressures and test the hypothesis that intracochlear pressure changes are proportional to the laser energy delivered.
Study design: Basic and translational science.
Setting: Cadaveric dissection and basic science laboratory.
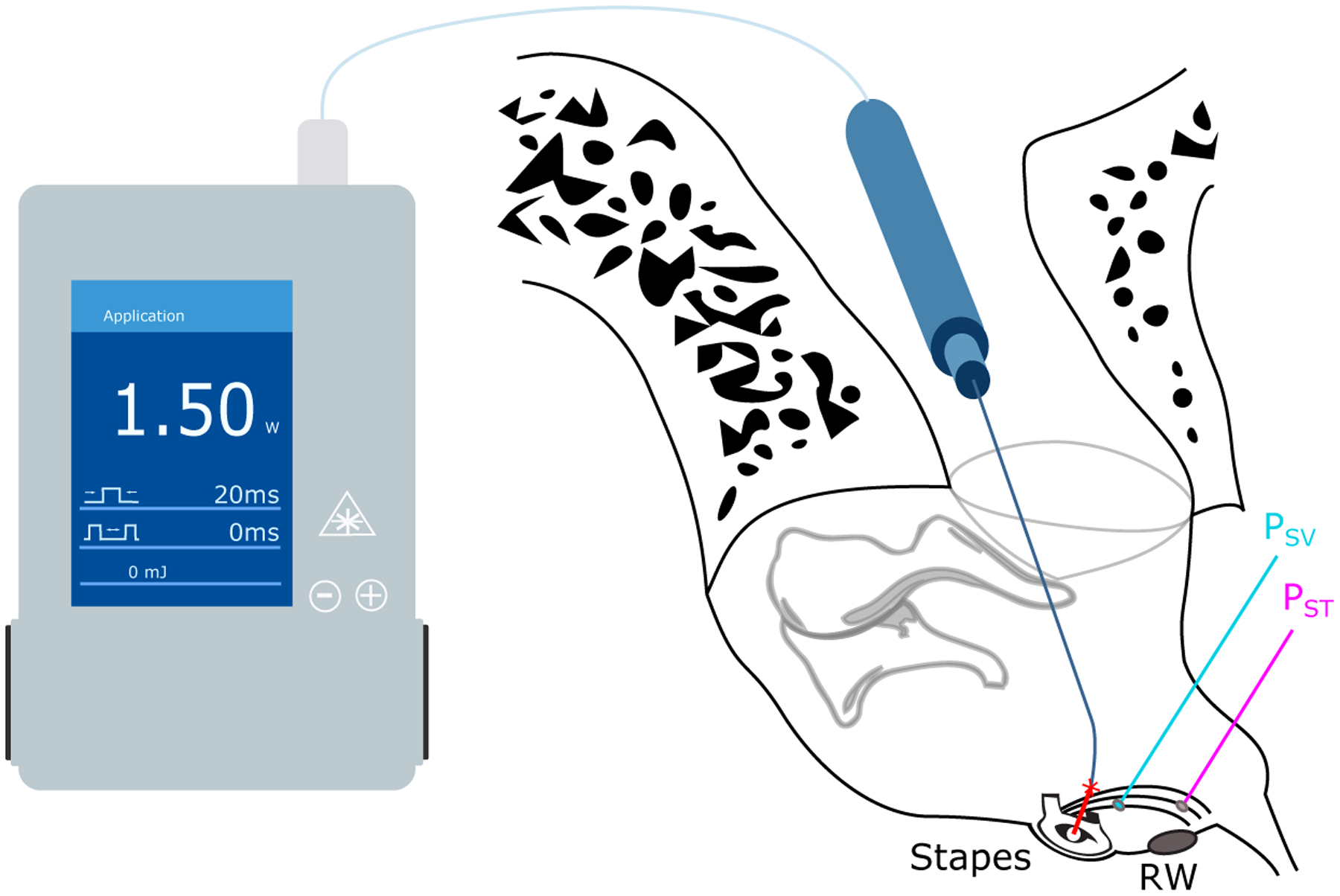
Methods: Cadaveric human heads underwent mastoidectomies. Intracochlear pressures were measured via fiber-optic pressure probes placed in scala vestibuli and tympani. Pulses of varied stimulus power and duration from a 980-nm diode laser were applied to the stapes footplate.
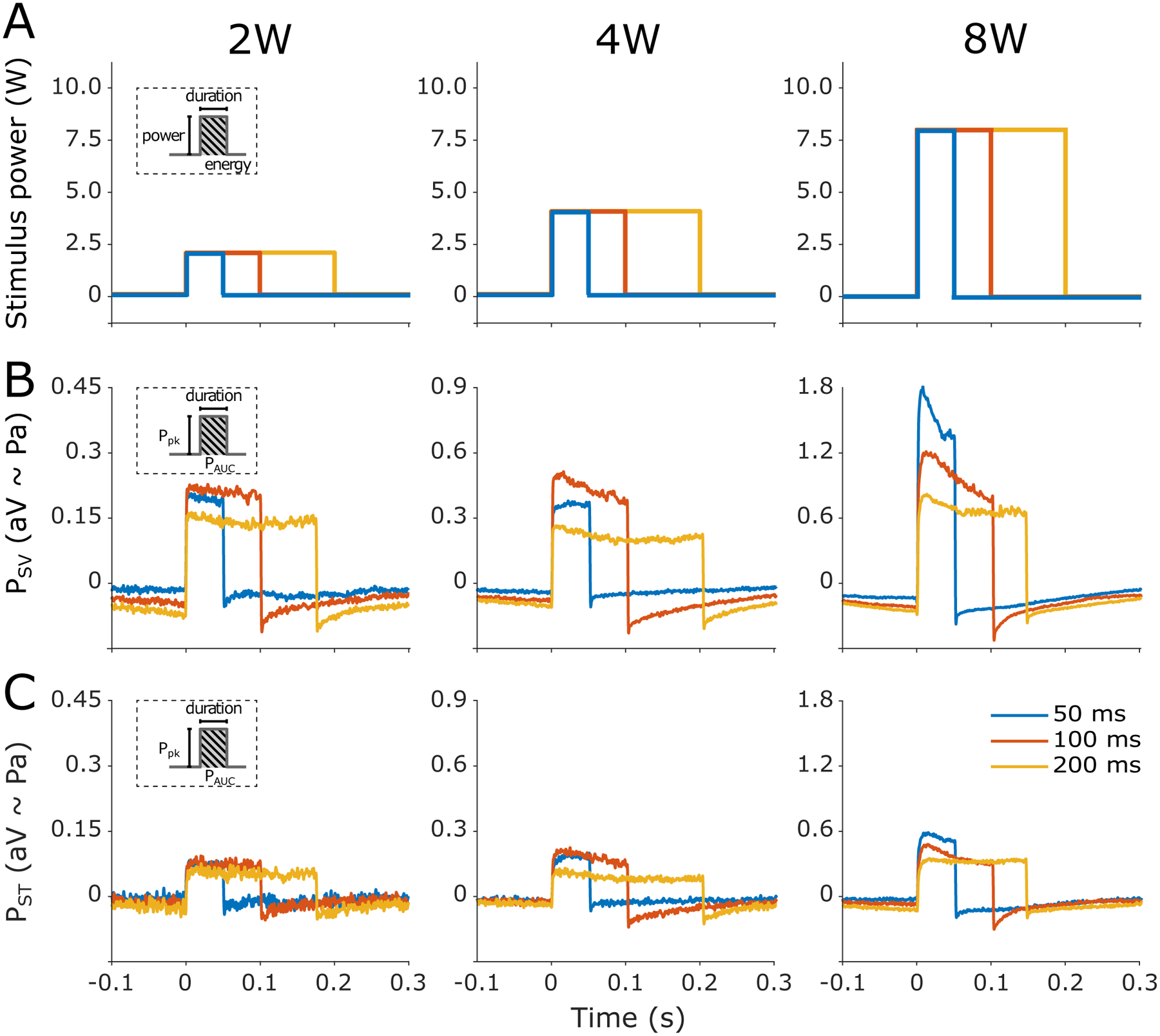
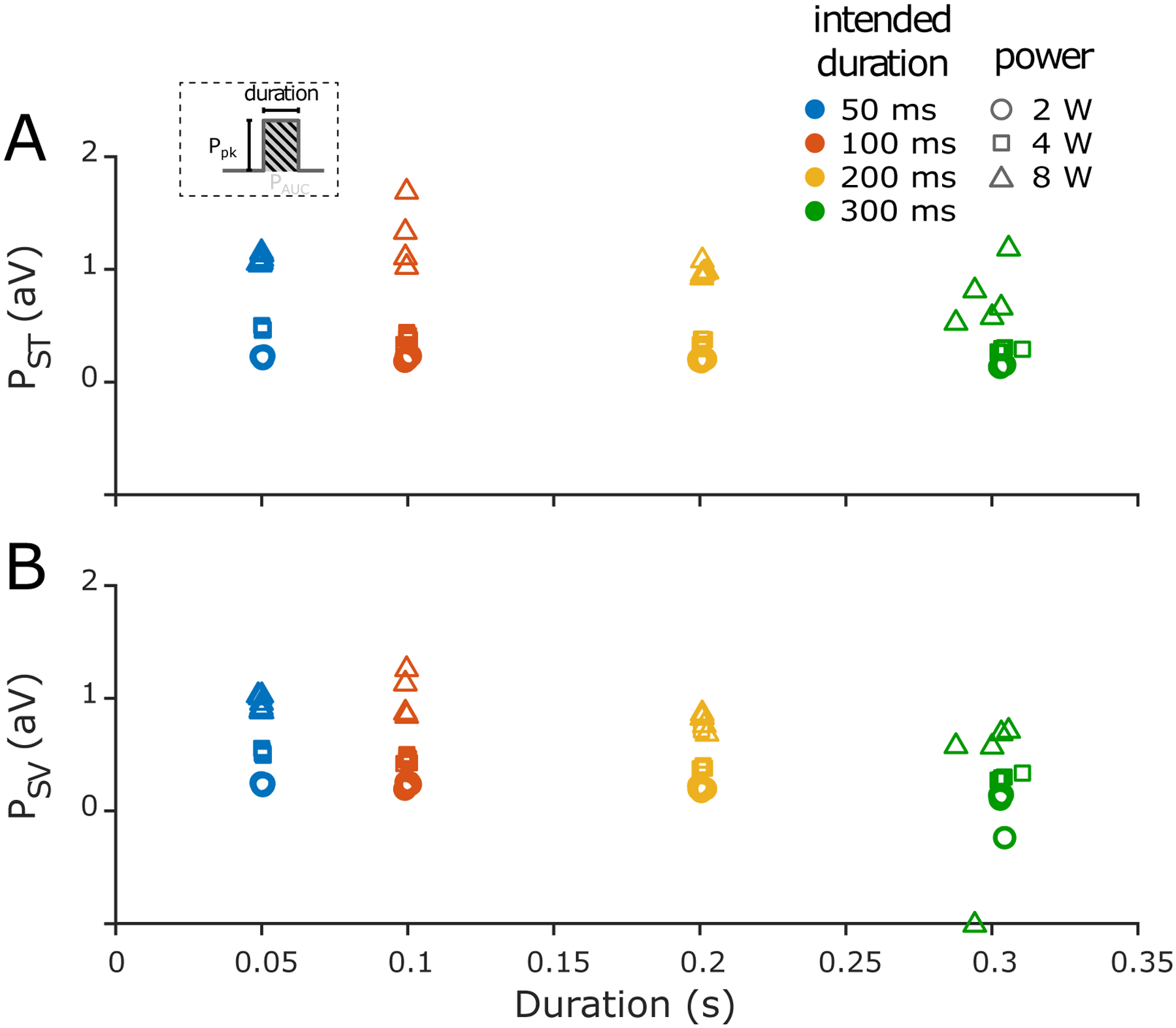
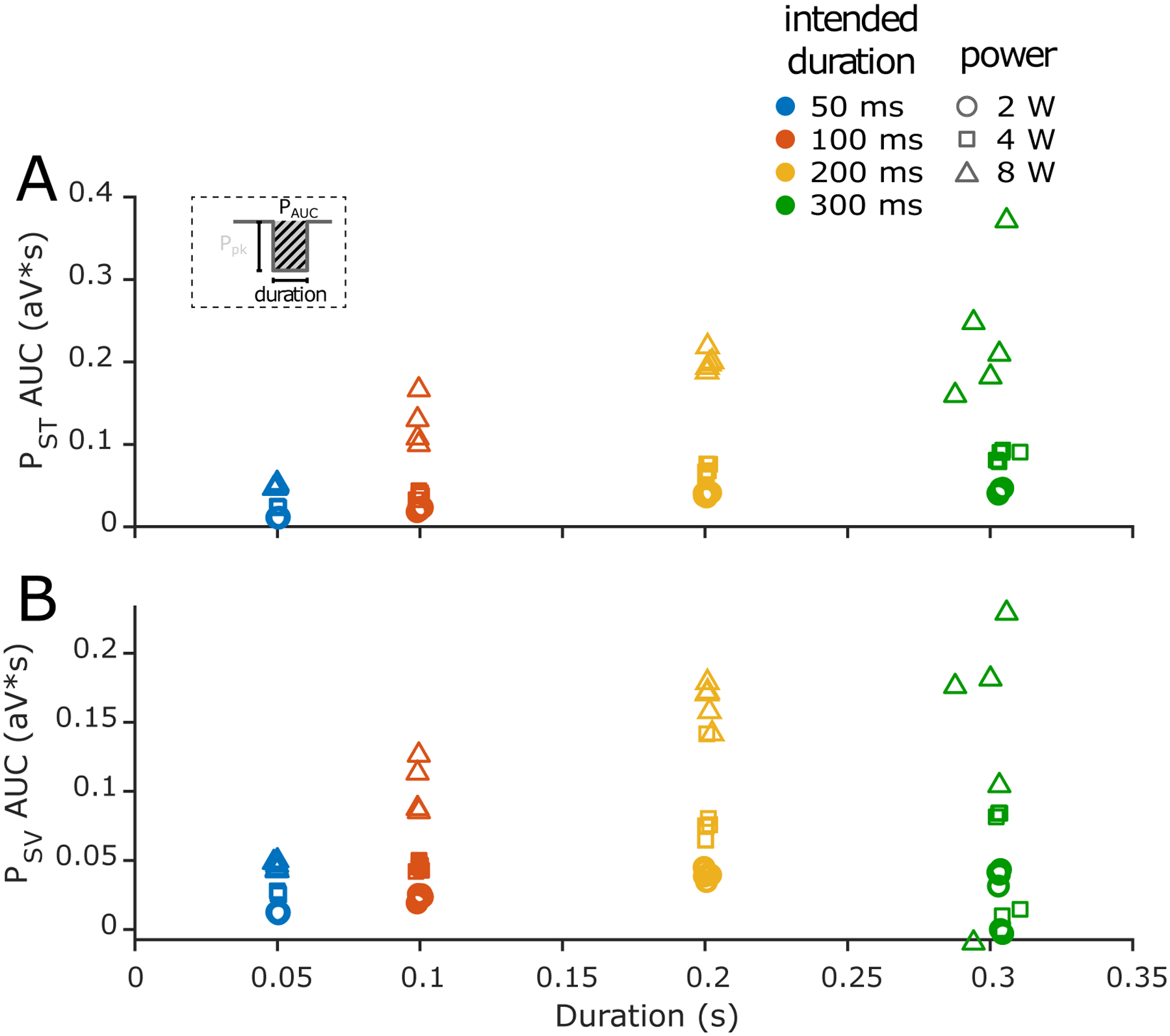
Results: Sustained high-intensity pressures were observed in the cochlea during all laser applications. Observed pressure magnitudes increased monotonically with laser energy and rose linearly for lower stimulus durations and powers, but there was increased variability for laser applications of longer duration (200-300 ms) and/or higher power (8 W).
Conclusions: Results confirm that significant pressure changes occur during laser stapedotomy, which we hypothesize may cause injury. Overall energy delivered depends predictably on duration and power, but surgeons should use caution at the highest stimulus levels and longest pulse durations due to the increasing variability in intracochlear pressure under these stimulus conditions. While the risk to hearing from increased intracochlear pressures from laser stapedotomy remains unclear, these results affirm the need to optimize laser settings to avoid unintended injury.
Keywords: intracochlear pressure; laser; noise-induced hearing loss; stapedectomy; stapedotomy.
© 2022 American Academy of Otolaryngology-Head and Neck Surgery Foundation.
Conflict of interest statement
Figures
Similar articles
-
Risks of Intracochlear Pressures From Laser Stapedotomy.Otol Neurotol. 2020 Mar;41(3):308-317. doi: 10.1097/MAO.0000000000002499. Otol Neurotol. 2020. PMID: 31746814 Free PMC article.
-
A Preliminary Investigation of the Air-Bone Gap: Changes in Intracochlear Sound Pressure With Air- and Bone-conducted Stimuli After Cochlear Implantation.Otol Neurotol. 2016 Oct;37(9):1291-9. doi: 10.1097/MAO.0000000000001184. Otol Neurotol. 2016. PMID: 27579835 Free PMC article.
-
Drill-induced Cochlear Injury During Otologic Surgery: Intracochlear Pressure Evidence of Acoustic Trauma.Otol Neurotol. 2017 Aug;38(7):938-947. doi: 10.1097/MAO.0000000000001474. Otol Neurotol. 2017. PMID: 28598950 Free PMC article.
-
Laser vs drill for footplate fenestration during stapedotomy: a systematic review and meta-analysis of hearing results.Eur Arch Otorhinolaryngol. 2021 Jan;278(1):9-14. doi: 10.1007/s00405-020-06117-1. Epub 2020 Jun 13. Eur Arch Otorhinolaryngol. 2021. PMID: 32535861
-
The Use of Lasers in Stapes Surgery.Ear Nose Throat J. 2021 Feb;100(1_suppl):73S-76S. doi: 10.1177/0145561320937828. Epub 2020 Jun 30. Ear Nose Throat J. 2021. PMID: 32603217 Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
