

Mesh deformation: A mechanism underlying polypropylene prolapse mesh complications in vivo
- PMID: 35671876
- PMCID: PMC9453339
- DOI: 10.1016/j.actbio.2022.05.051
Mesh deformation: A mechanism underlying polypropylene prolapse mesh complications in vivo
Abstract
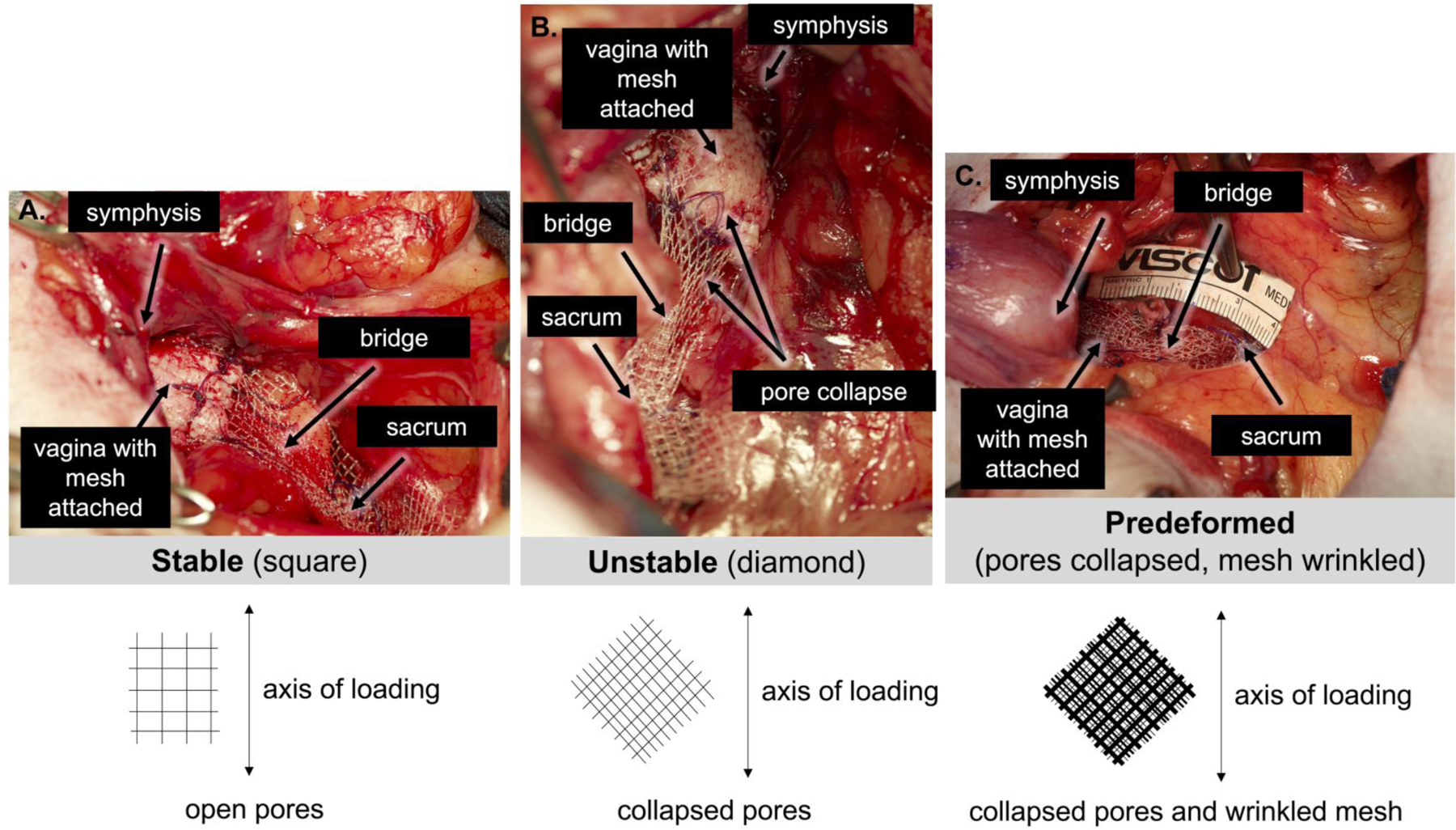
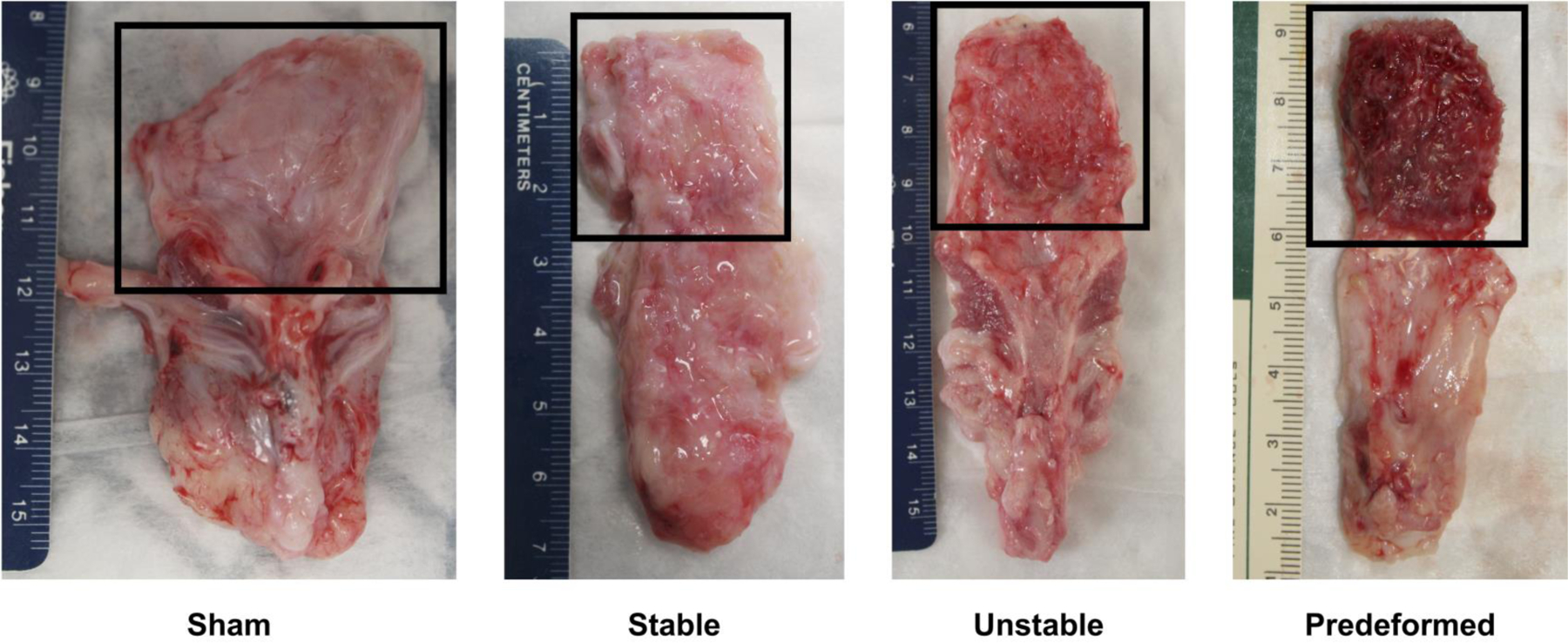
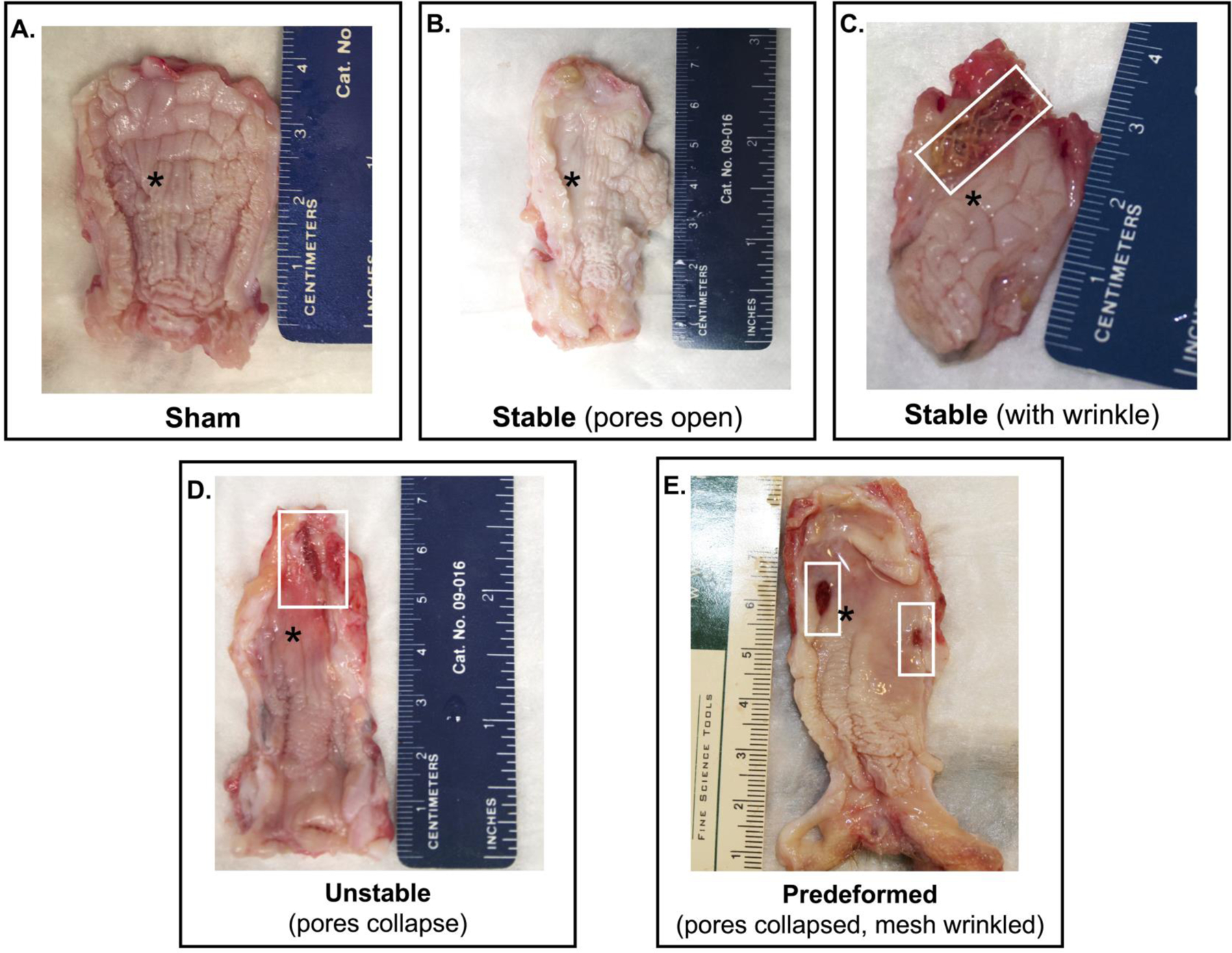
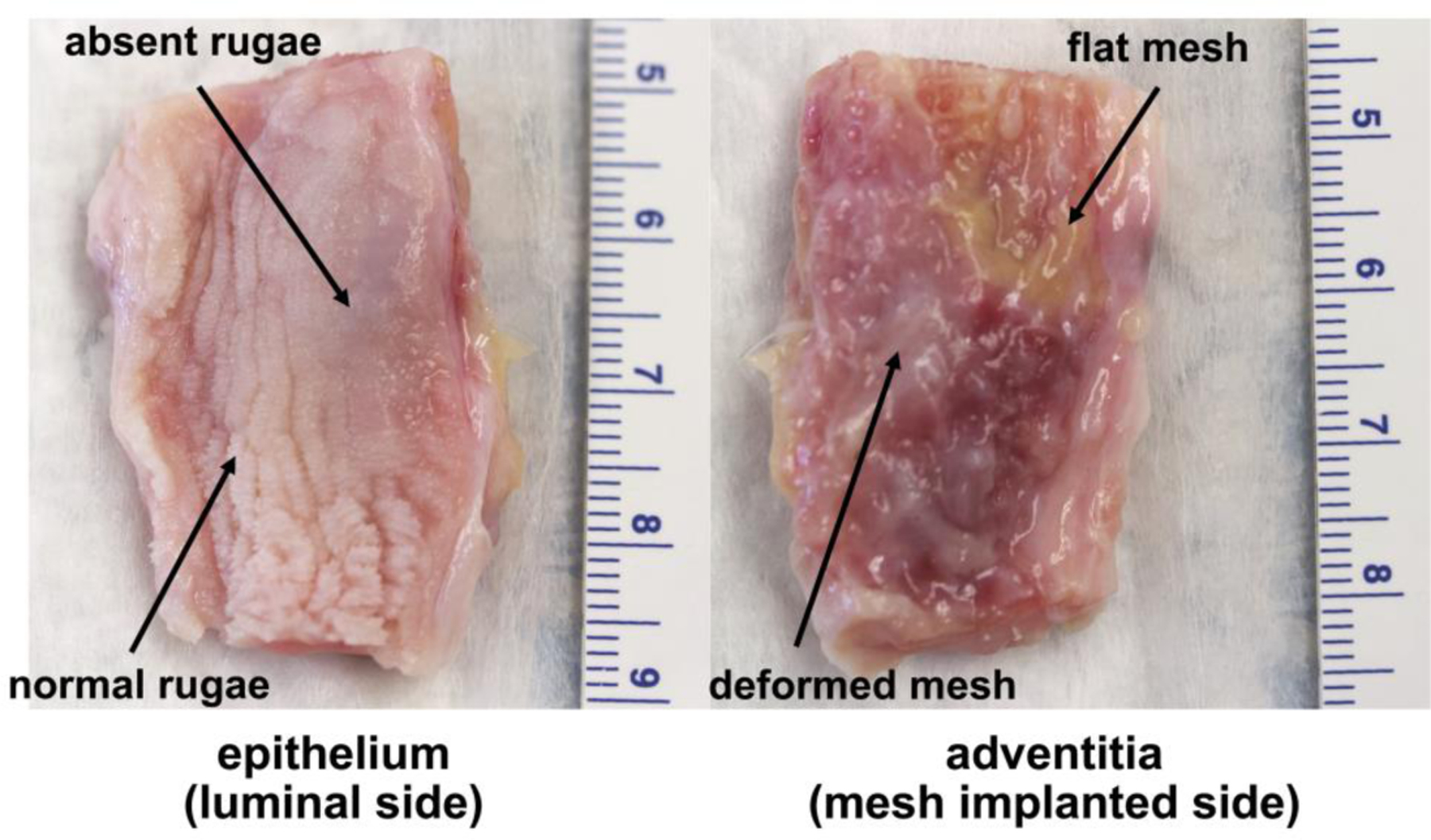
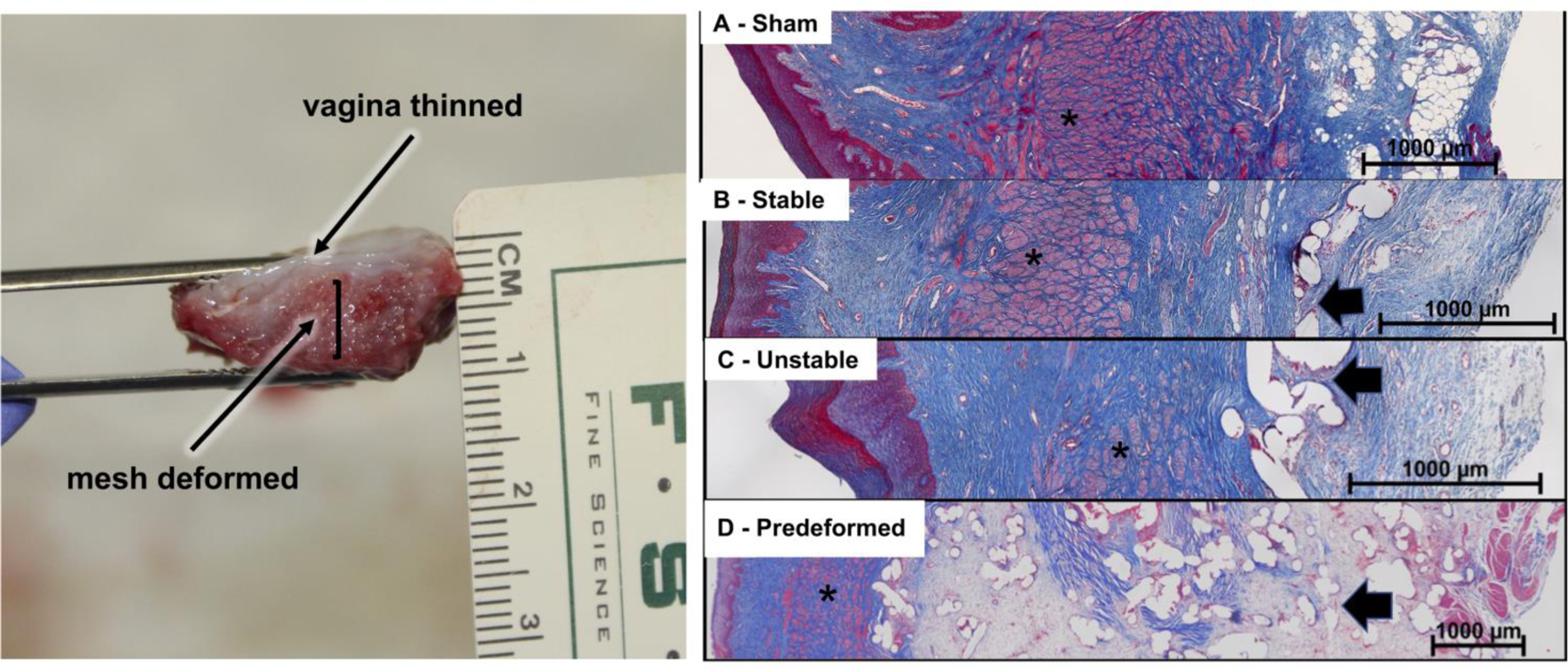
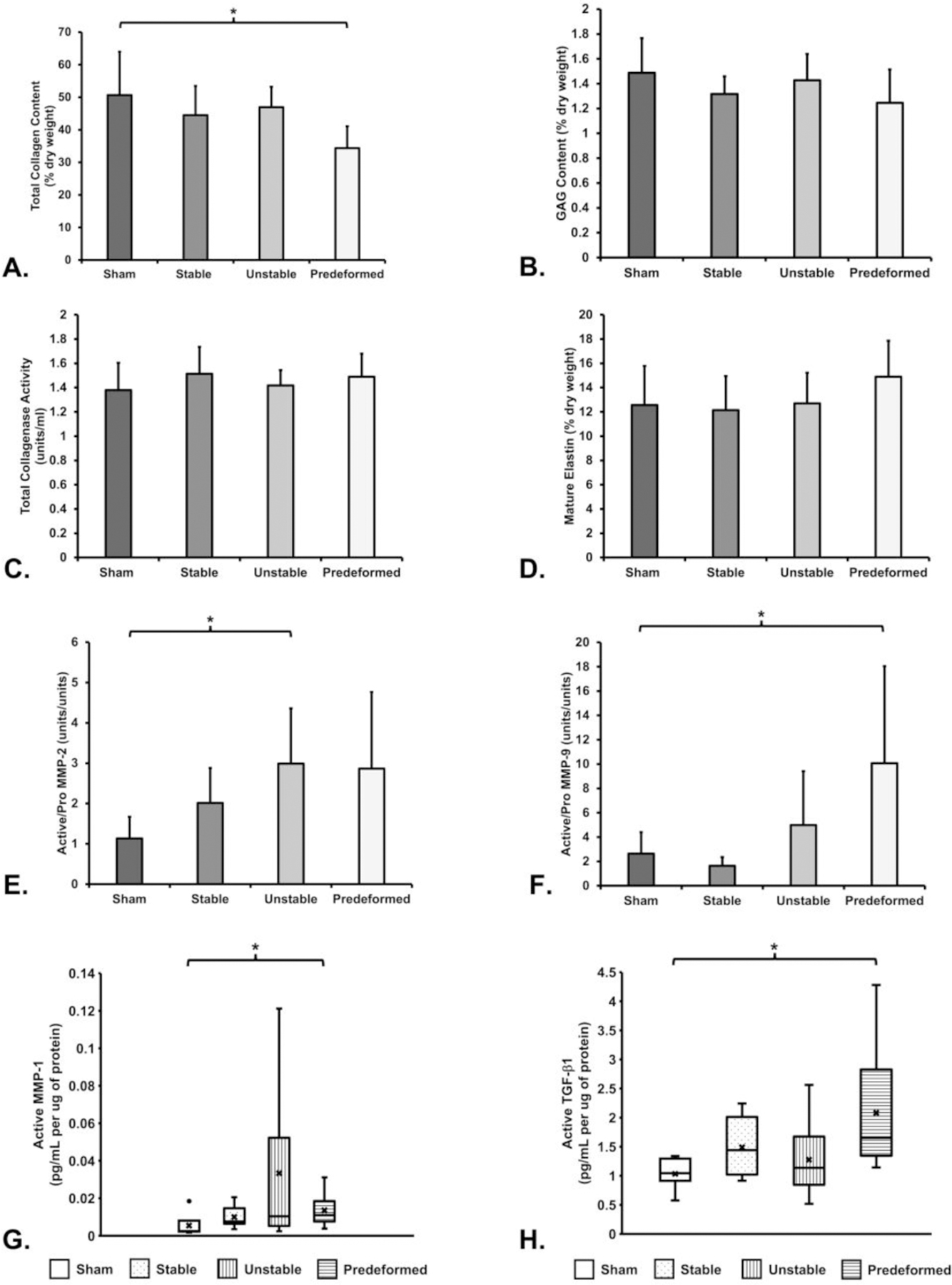
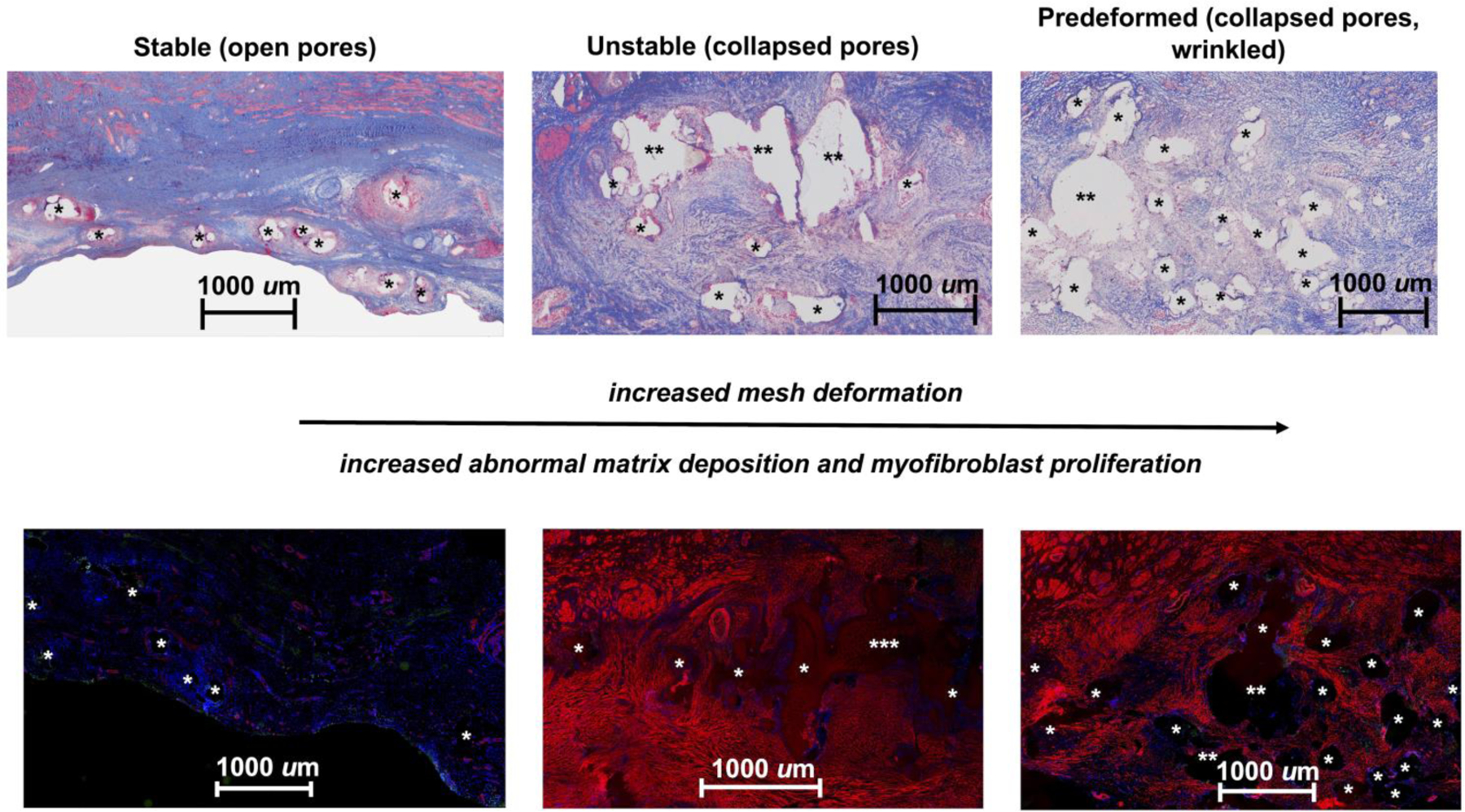
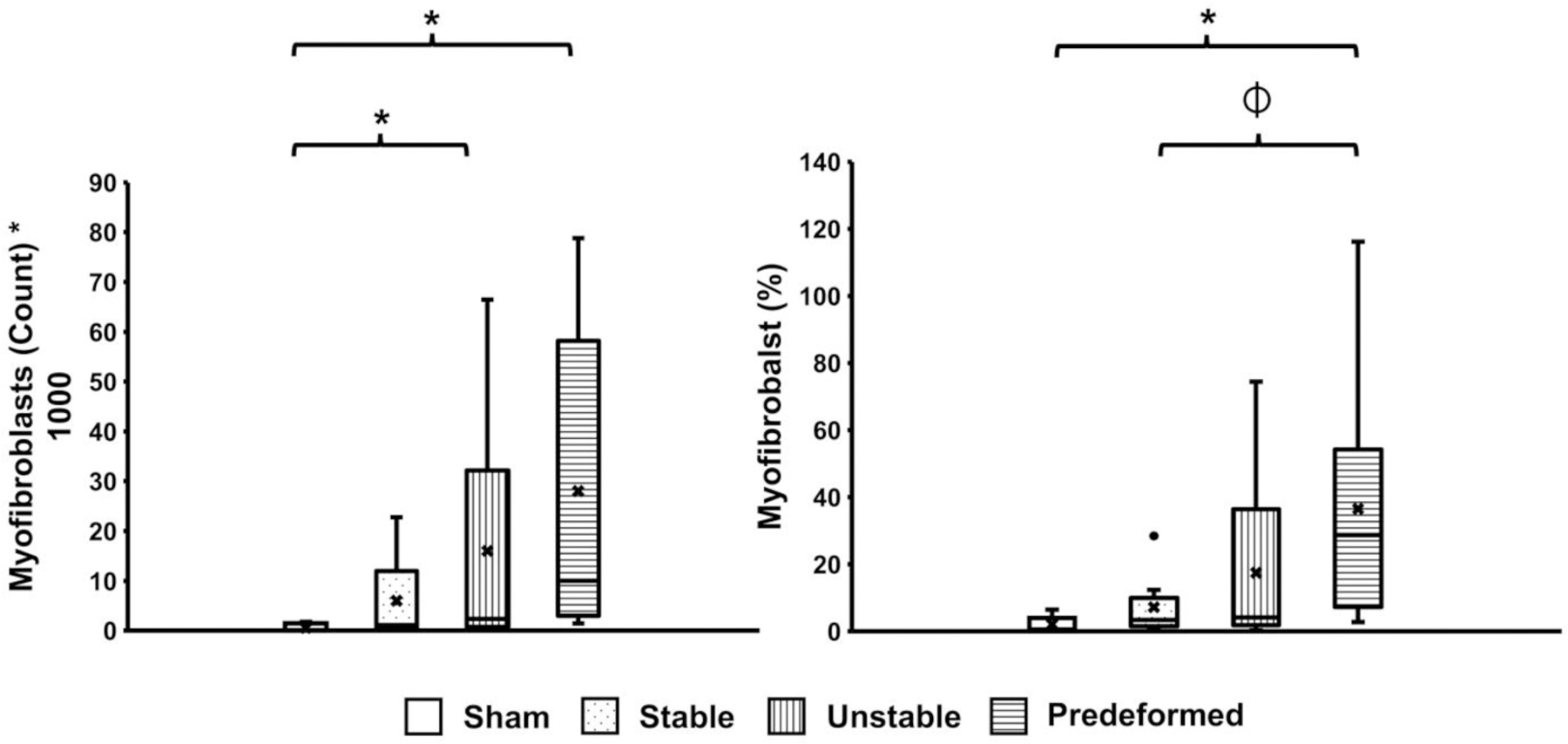
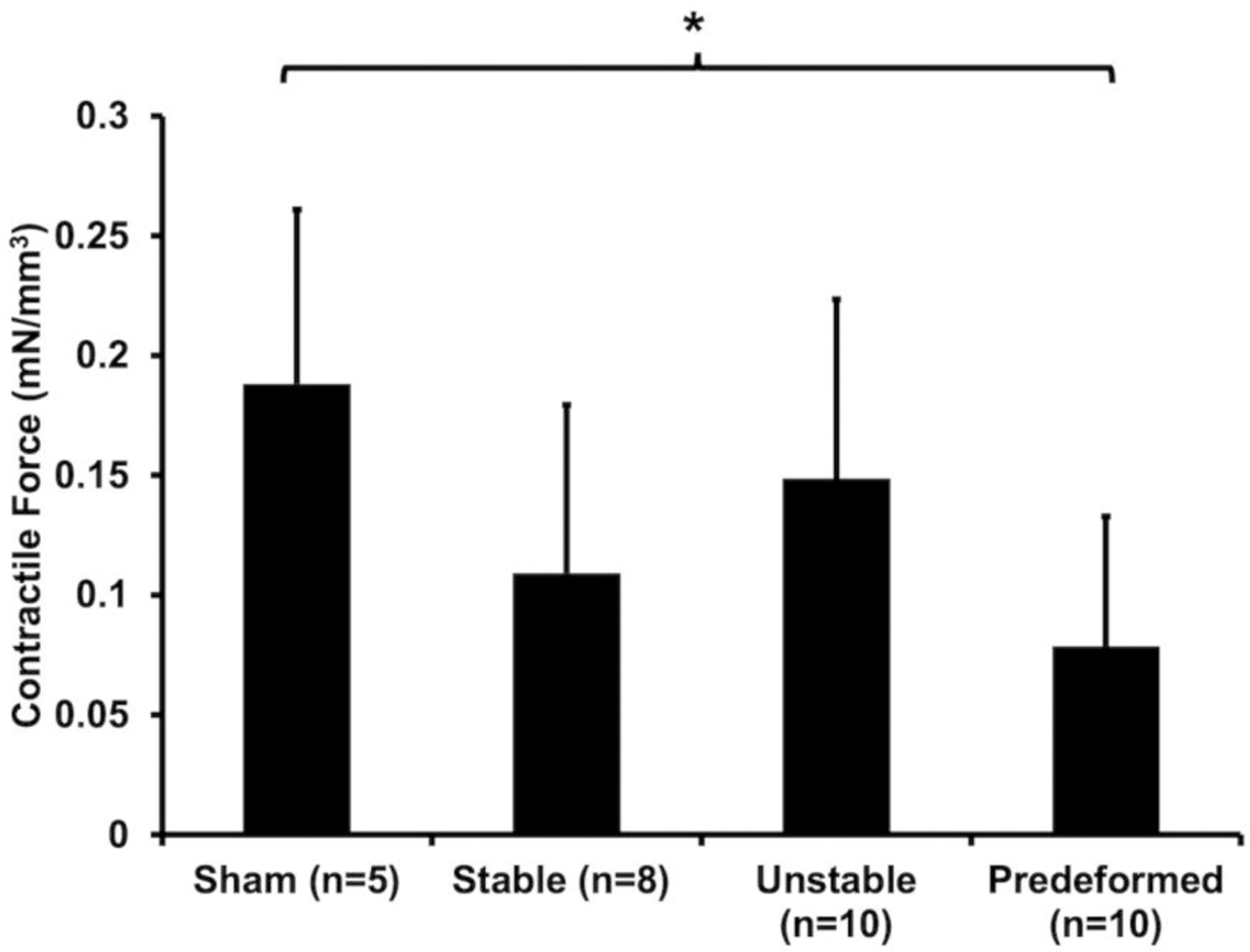
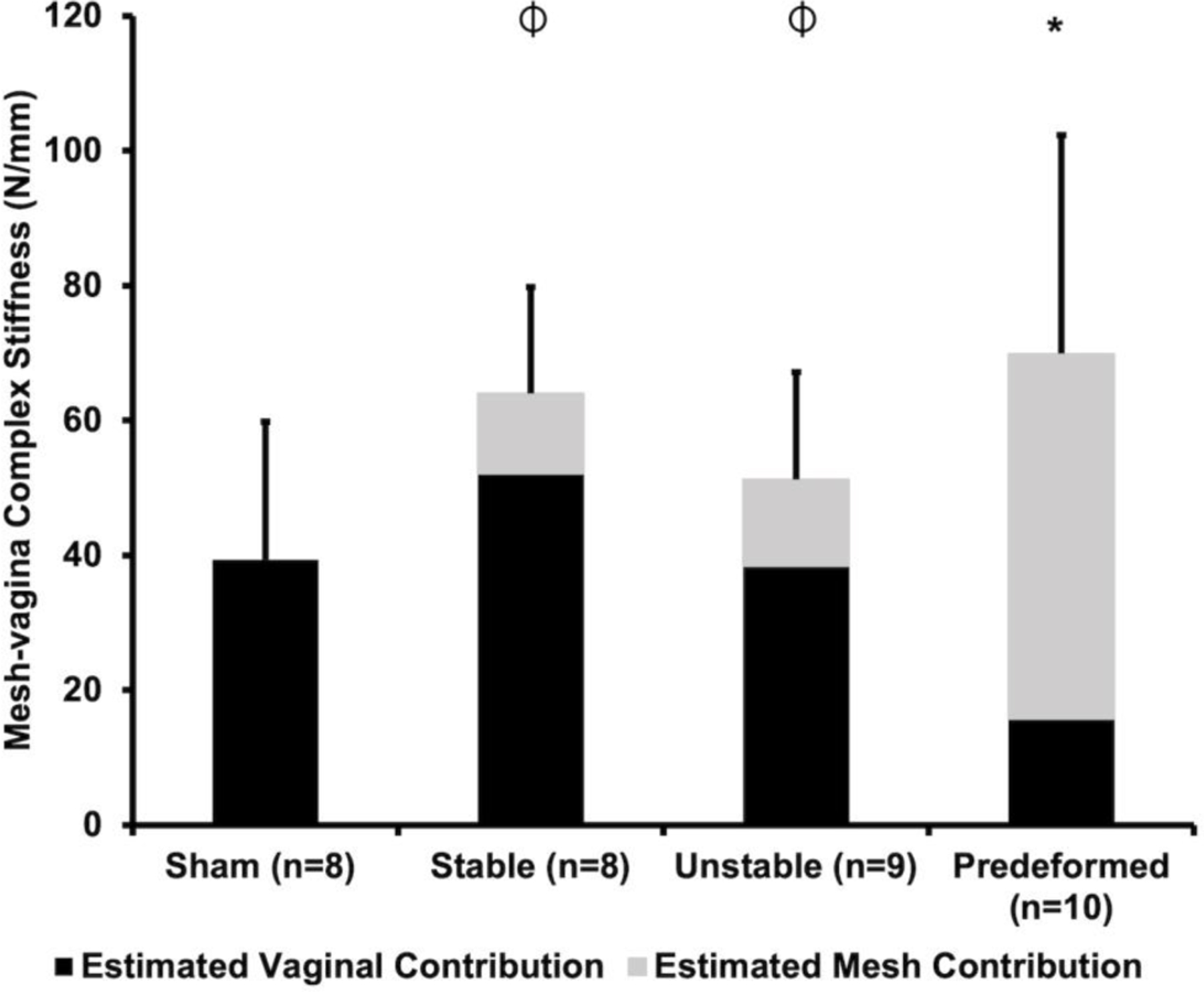
Polypropylene meshes used in pelvic organ prolapse (POP) repair are hampered by complications. Most POP meshes are highly unstable after tensioning ex vivo, as evidenced by marked deformations (pore collapse and wrinkling) that result in altered structural properties and material burden. By intentionally introducing collapsed pores and wrinkles into a mesh that normally has open pores and remains relatively flat after implantation, we reproduce mesh complications in vivo. To do this, meshes were implanted onto the vagina of rhesus macaques in nondeformed (flat) vs deformed (pore collapse +/- wrinkles) configurations and placed on tension. Twelve weeks later, animals with deformed meshes had two complications, (1) mesh exposure through the vaginal epithelium, and (2) myofibroblast proliferation with fibrosis - a mechanism of pain. The overarching response to deformed mesh was vaginal thinning associated with accelerated apoptosis, reduced collagen content, increased proteolysis, deterioration of mechanical integrity, and loss of contractile function consistent with stress shielding - a precursor to mesh exposure. Regional differences were observed, however, with some areas demonstrating myofibroblast proliferation and matrix deposition. Variable mechanical cues imposed by deformed meshes likely induce these two disparate responses. Utilizing meshes associated with uniform stresses on the vagina by remaining flat with open pores after tensioning is critical to improving outcomes. STATEMENT OF SIGNIFICANCE: Pain and exposure are the two most reported complications associated with the use of polypropylene mesh in urogynecologic procedures. Most meshes have unstable geometries as evidenced by pore collapse and wrinkling after tensioning ex vivo, recapitulating what is observed in meshes excised from women with complications in vivo. We demonstrate that collapsed pores and wrinkling result in two distinct responses (1) mesh exposure associated with tissue degradation and atrophy and (2) myofibroblast proliferation and matrix deposition consistent with fibrosis, a tissue response associated with pain. In conclusion, mesh deformation leads to areas of tissue degradation and myofibroblast proliferation, the likely mechanisms of mesh exposure and pain, respectively. These data corroborate that mesh implantation in a flat configuration with open pores is a critical factor for reducing complications in mesh-augmented surgeries.
Keywords: Biomechanical properties; Extracellular matrix; Stress shielding; Synthetic mesh complications; Vagina.
Copyright © 2022. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. We would like to draw the attention of the Editor to the following facts which may be considered as potential declaration of interests: Pamela A. Moalli reports equipment, drugs, or supplies was provided by Coloplast Corp. Katrina M. Knight reports financial support was provided by Magee-Womens Research Institute & Foundation. Pamela A. Moalli reports a relationship with Hologic Inc that includes: board membership. However, there has been no significant financial support for this work that could have influenced its outcome.
Figures
References
-
- Samuelsson EC, Victor A, Tibblin G, Svardsudd KF, Signs of genital prolapse in a Swedish population of women 20 to 59 years of age and possible related factors, American Journal of Obstetrics and Gynecology 180(2 I) (1999) 299–305. - PubMed
-
- Barber MD, Brubaker L, Burgio KL, Richter HE, Nygaard I, Weidner AC, Menefee SA, Lukacz ES, Norton P, Schaffer J, Nguyen JN, Borello-France D, Goode PS, Jakus-Waldman S, Spino C, Warren LK, Gantz MG, Meikle SF, Comparison of 2 transvaginal surgical approaches and perioperative behavioral therapy for apical vaginal prolapse: The OPTIMAL randomized trial, JAMA - Journal of the American Medical Association 311(10) (2014) 1023–1034. - PMC - PubMed
-
- Jelovsek JE, Barber MD, Norton P, Brubaker L, Gantz M, Richter HE, Weidner A, Menefee S, Schaffer J, Pugh N, Meikle S, Effect of uterosacral ligament suspension vs sacrospinous ligament fixation with or without perioperative behavioral therapy for pelvic organ vaginal prolapse on surgical outcomes and prolapse symptoms at 5 years in the OPTIMAL randomized clinical trial, JAMA - Journal of the American Medical Association 319(15) (2018) 1554–1565. - PMC - PubMed
-
- U.S.F.a.D. Administration, Surgical Mesh for Treatment of Women with Pelvic Organ Prolapse and Stress Urinary Incontinence: FDA Executive Summary, 2011.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
