

Political environment and mortality rates in the United States, 2001-19: population based cross sectional analysis
- PMID: 35672032
- PMCID: PMC9171631
- DOI: 10.1136/bmj-2021-069308
Political environment and mortality rates in the United States, 2001-19: population based cross sectional analysis
Abstract
Objective: To assess recent trends in age adjusted mortality rates (AAMRs) in the United States based on county level presidential voting patterns.
Design: Cross sectional study.
Setting: USA, 2001-19.
Participants: 99.8% of the US population.
Main outcome measures: AAMR per 100 000 population and average annual percentage change (APC).
Methods: The Centers for Disease Control and Prevention WONDER database was linked to county level data on US presidential elections. County political environment was classified as either Democratic or Republican for the four years that followed a November presidential election. Additional sensitivity analyses analyzed AAMR trends for counties that voted only for one party throughout the study, and county level gubernatorial election results and state level AAMR trends. Joinpoint analysis was used to assess for an inflection point in APC trends.
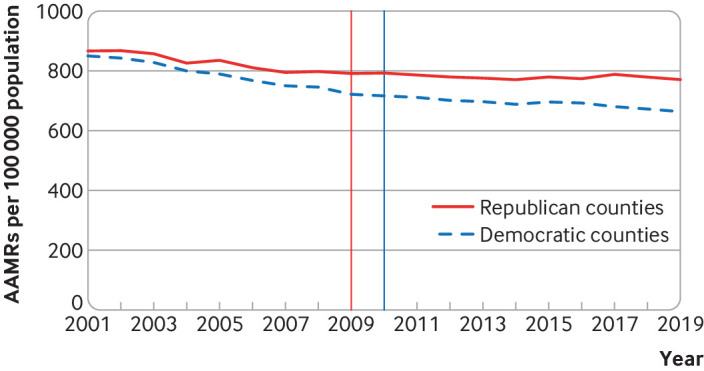
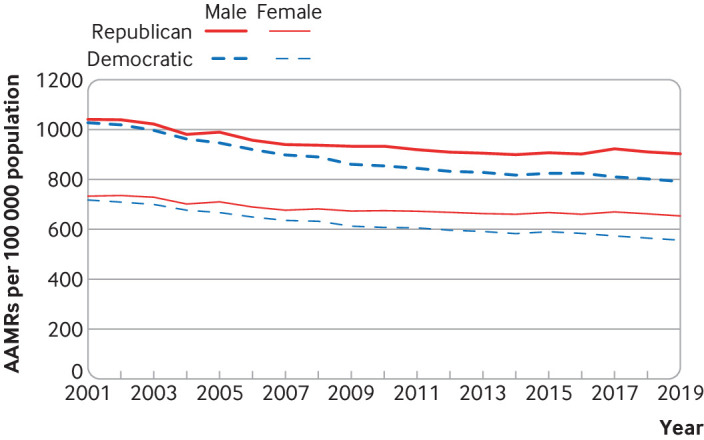
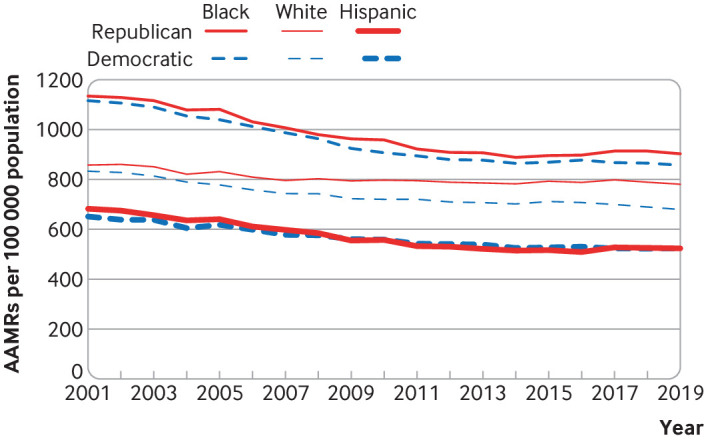
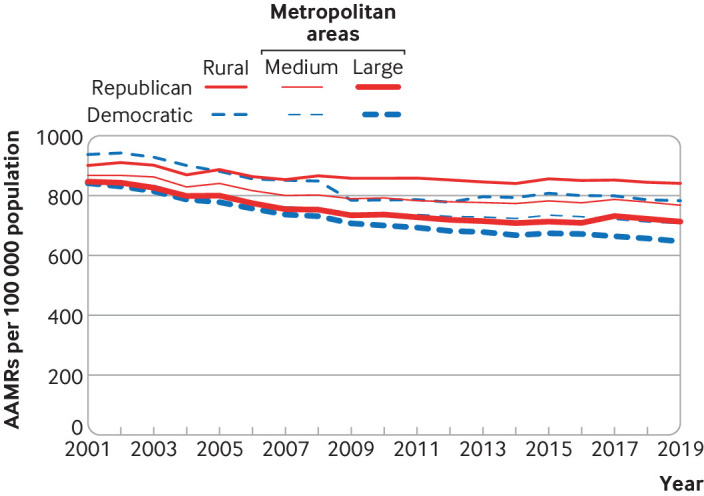
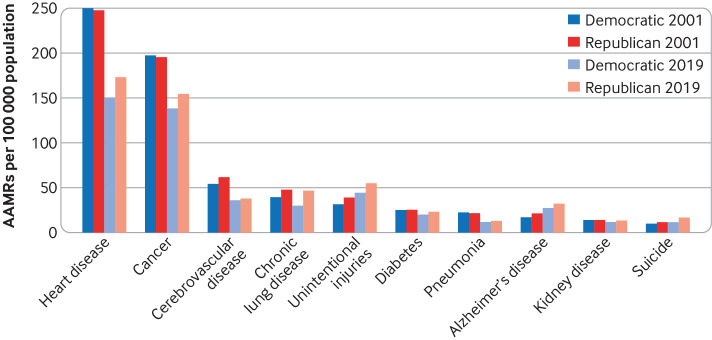
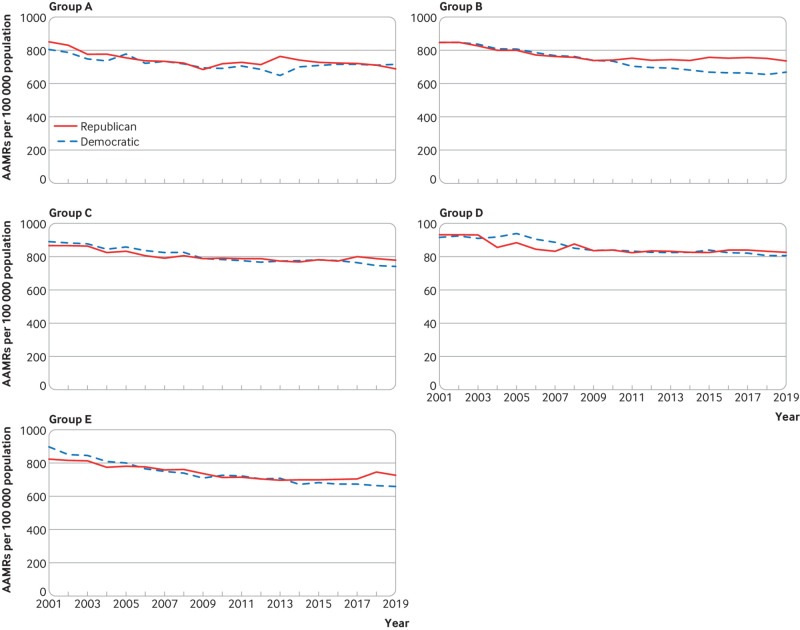
Results: The study period covered five presidential elections from 2000 to 2019. From 2001 to 2019, the AAMR per 100 000 population decreased by 22% in Democratic counties, from 850.3 to 664.0 (average APC -1.4%, 95% confidence interval -1.5% to -1.2%), but by only 11% in Republican counties, from 867.0 to 771.1 (average APC -0.7%, -0.9% to -0.5%). The gap in AAMR between Democratic and Republican counties therefore widened from 16.7 (95% confidence interval 16.6 to 16.8) to 107.1 (106.5 to 107.7). Statistically significant inflection points in APC occurred for Democratic counties between periods 2001-09 (APC -2.1%, -2.3% to -1.9%) and 2009-19 (APC -0.8%, -1.0% to -0.6%). For Republican counties between 2001 and 2008 the APC was -1.4% (-1.8% to -1.0%), slowing to near zero between 2008 and 2019 (APC -0.2%, -0.4% to 0.0%). Male and female residents of Democratic counties experienced both lower AAMR and twice the relative decrease in AAMR than did those in Republican counties. Black Americans experienced largely similar improvement in AAMR in both Democratic and Republican counties. However, the AAMR gap between white residents in Democratic versus Republican counties increased fourfold, from 24.7 (95% confidence interval 24.6 to 24.8) to 101.3 (101.0 to 101.6). Rural Republican counties experienced the highest AAMR and the least improvement. All trends were similar when comparing counties that did not switch political environment throughout the period and when gubernatorial election results were used. The greatest contributors to the widening AAMR gap between Republican and Democratic counties were heart disease (difference in AAMRs 27.6), cancer (17.3), and chronic lower respiratory tract diseases (8.3), followed by unintentional injuries (3.3) and suicide (3.0).
Conclusion: The mortality gap in Republican voting counties compared with Democratic voting counties has grown over time, especially for white populations, and that gap began to widen after 2008.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: HW is an advisor for Embrace Prevention Care; RW receives research support from the National Heart, Lung, and Blood Institute (grant K23HL148525-1); KEJM previously did contract work for the US Department of Health and Human Services; no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Politics and mortality in the United States.BMJ. 2022 Jun 7;377:o1308. doi: 10.1136/bmj.o1308. BMJ. 2022. PMID: 35672047 No abstract available.
Similar articles
-
Independent Relationship of Changes in Death Rates with Changes in US Presidential Voting.J Gen Intern Med. 2019 Mar;34(3):363-371. doi: 10.1007/s11606-018-4568-6. Epub 2018 Sep 5. J Gen Intern Med. 2019. PMID: 30187378 Free PMC article.
-
Swing voting in the 2016 presidential election in counties where midlife mortality has been rising in white non-Hispanic Americans.Soc Sci Med. 2018 Jan;197:33-38. doi: 10.1016/j.socscimed.2017.11.050. Epub 2017 Dec 2. Soc Sci Med. 2018. PMID: 29220706
-
Diverging Life Expectancies and Voting Patterns in the 2016 US Presidential Election.Am J Public Health. 2017 Oct;107(10):1560-1562. doi: 10.2105/AJPH.2017.303945. Epub 2017 Aug 17. Am J Public Health. 2017. PMID: 28817322 Free PMC article.
-
Demographics and Trends of Hypertrophic Cardiomyopathy-Related Mortality in the United States, 1999-2020.Curr Probl Cardiol. 2023 Jul;48(7):101681. doi: 10.1016/j.cpcardiol.2023.101681. Epub 2023 Mar 10. Curr Probl Cardiol. 2023. PMID: 36906160 Review.
-
Physical Inactivity and Obesity in the United States Through the Lens of the 2012 and 2016 Presidential Elections.Curr Probl Cardiol. 2024 Jan;49(1 Pt B):102068. doi: 10.1016/j.cpcardiol.2023.102068. Epub 2023 Sep 7. Curr Probl Cardiol. 2024. PMID: 37689376 Review.
Cited by
-
Geographic access to pediatric neurosurgeons in the USA: an analysis of sociodemographic factors.Childs Nerv Syst. 2024 Mar;40(3):905-912. doi: 10.1007/s00381-023-06172-z. Epub 2023 Oct 4. Childs Nerv Syst. 2024. PMID: 37794171 Free PMC article.
-
Politicians, power, and the people's health: US elections and state health outcomes, 2012-2024.Health Aff Sch. 2024 Nov 27;2(12):qxae163. doi: 10.1093/haschl/qxae163. eCollection 2024 Dec. Health Aff Sch. 2024. PMID: 39664487 Free PMC article.
-
Threats to Democracy and the Right to Health.Am J Public Health. 2025 Mar;115(3):307-309. doi: 10.2105/AJPH.2024.307992. Am J Public Health. 2025. PMID: 39938035 Free PMC article. No abstract available.
-
American election results at the precinct level.Sci Data. 2022 Nov 3;9(1):651. doi: 10.1038/s41597-022-01745-0. Sci Data. 2022. PMID: 36329037 Free PMC article.
-
Community-level age bias and older adult mortality.Soc Sci Med. 2023 Jan;317:115449. doi: 10.1016/j.socscimed.2022.115449. Epub 2022 Nov 21. Soc Sci Med. 2023. PMID: 36494219 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous