

Sociodemographic characteristics and emergency department visits and inpatient hospitalizations for atopic dermatitis in Ontario: a cross-sectional study
- PMID: 35672041
- PMCID: PMC9177197
- DOI: 10.9778/cmajo.20210194
Sociodemographic characteristics and emergency department visits and inpatient hospitalizations for atopic dermatitis in Ontario: a cross-sectional study
Abstract
Background: Some jurisdictions experience sociodemographic disparities in atopic dermatitis care, including emergency department visits, but data from Canada are limited. Our objectives were to estimate the prevalence of atopic dermatitis in Ontario and to identify sociodemographic factors associated with emergency department visits and hospitalizations for this condition.
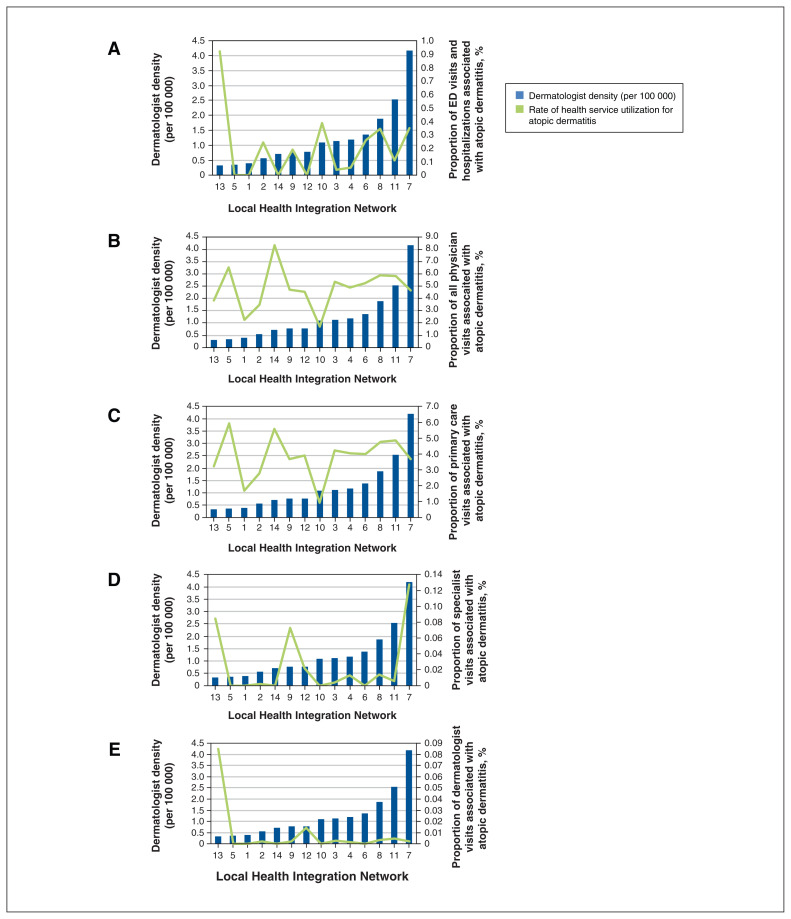
Methods: We conducted a cross-sectional analysis of patients in the Electronic Medical Record Primary Care database linked with administrative health data for Ontario, Canada. We estimated period prevalence and health service utilization for atopic dermatitis from 2005 to 2015. We used multivariable log-binomial regression to calculate adjusted risk ratios (RRs) and 95% confidence intervals (CIs) for associations between local dermatologist density and the proportion of emergency department visits and hospitalizations for atopic dermatitis.
Results: Among 249 984 patients, we identified 7812 with atopic dermatitis (period prevalence 2005-2015: 3.1%). Almost all physician visits for atopic dermatitis were to primary care physicians (> 99%). For every additional dermatologist per 100 000 population, the proportions of emergency department visits and hospitalizations for atopic dermatitis increased by 29% (RR 1.29, 95% CI 1.05-1.57). This relationship occurred in and around Toronto but was not consistent across the province.
Interpretation: In Ontario, higher dermatologist density was not associated with lower emergency department utilization and hospitalization for atopic dermatitis; the association varied in different locales with similar dermatologist densities. Strategies to improve access to care for atopic dermatitis should be tailored to local contexts.
© 2022 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests: Aaron Drucker has received compensation from the British Journal of Dermatology (reviewer and section editor), the American Academy of Dermatology (guidelines writer) and the National Eczema Association (grant reviewer); he has been a paid consultant for the Canadian Agency for Drugs and Technologies in Health; and he has received research grants (to his institution) from the Canadian Dermatology Foundation, the PSI Foundation and the Canadian Institutes for Health Research. Lihi Eder received research and educational grants from Novartis, AbbVie, Sandoz, Pfizer, Eli Lilly, Janssen, Fresenius Kabi and UCB; consulting fees from Novartis, Eli Lilly, Janssen, AbbVie and Pfizer; and honoraria from Novartis and AbbVie. Elena Pope received royalties from UpToDate, has been an investigator for Pierre-Fabre Pharmaceuticals, Galderma, and Maine Pharma, and an advisory board member for Novartis, Boehringer-Ingelheim and Pfizer; she has served as an executive board member and chair of the communication committee of the Pediatric Dermatology Research Alliance, and chair of the strategic committee of the Society for Pediatric Dermatology. Karen Tu has received grants paid to her institution from St. Michael’s Hospital Foundation, the College of Family Physicians of Canada, the Foundation for Advancing Family Medicine, the Canadian Medical Association Foundation, North York General Hospital, the Heart and Stroke Foundation of Canada, the Heart and Stroke Foundation of Ontario, the United States Department of Defense, the University of Toronto Department of Family and Community Medicine, the MaRS Innovation Fund, the Canadian Initiative for Outcomes in Rheumatology Care, Cancer Care Ontario, the Toronto Rehab Institute Chair Fund, UTOPIAN, the Arthritis Society, the Multiple Sclerosis Society of Canada, the Canadian Vascular Network and the Ontario SPOR Support Unit Targeted IMPACT Award. No other competing interests declared.
Figures

Similar articles
-
Hospitalizations and emergency department visits for psychiatric illness during and after pregnancy among women with schizophrenia.J Clin Psychiatry. 2016 Apr;77(4):541-7. doi: 10.4088/JCP.14m09697. J Clin Psychiatry. 2016. PMID: 27035409
-
Healthcare Service Utilization by 116,816 Patients with Atopic Dermatitis in Israel.Acta Derm Venereol. 2019 Apr 1;99(4):370-374. doi: 10.2340/00015555-3117. Acta Derm Venereol. 2019. PMID: 30666336
-
Trends in health service use among persons with Parkinson's disease by rurality: A population-based repeated cross-sectional study.PLoS One. 2023 May 19;18(5):e0285585. doi: 10.1371/journal.pone.0285585. eCollection 2023. PLoS One. 2023. PMID: 37205650 Free PMC article.
-
Clarifying rural-urban disparities in alcohol-related emergency department visits and hospitalizations in Ontario, Canada: A spatial analysis.J Rural Health. 2023 Jan;39(1):223-232. doi: 10.1111/jrh.12702. Epub 2022 Jul 22. J Rural Health. 2023. PMID: 35866637
-
Temporal Trends and Predictors of Thirty-Day Readmissions and Emergency Department Visits Following Total Knee Arthroplasty in Ontario Between 2003 and 2016.J Arthroplasty. 2020 Feb;35(2):364-370. doi: 10.1016/j.arth.2019.09.015. Epub 2019 Sep 14. J Arthroplasty. 2020. PMID: 31732370 Review.
Cited by
-
Knowledge assessment tools in atopic dermatitis patient education: a scoping review.Allergy Asthma Clin Immunol. 2025 May 24;21(1):26. doi: 10.1186/s13223-025-00970-7. Allergy Asthma Clin Immunol. 2025. PMID: 40413499 Free PMC article. Review.
References
-
- Silverberg JI, Garg NK, Paller AS, et al. Sleep disturbances in adults with eczema are associated with impaired overall health: a US population-based study. J Invest Dermatol. 2015;135:56–66. - PubMed
-
- Kwa L, Silverberg JI. Financial burden of emergency department visits for atopic dermatitis in the United States. J Am Acad Dermatol. 2018;79:443–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources