

Cisternostomy for malignant middle cerebral artery infarction: proposed pathophysiological mechanisms and preliminary results
- PMID: 35672081
- PMCID: PMC9811554
- DOI: 10.1136/svn-2021-000918
Cisternostomy for malignant middle cerebral artery infarction: proposed pathophysiological mechanisms and preliminary results
Abstract
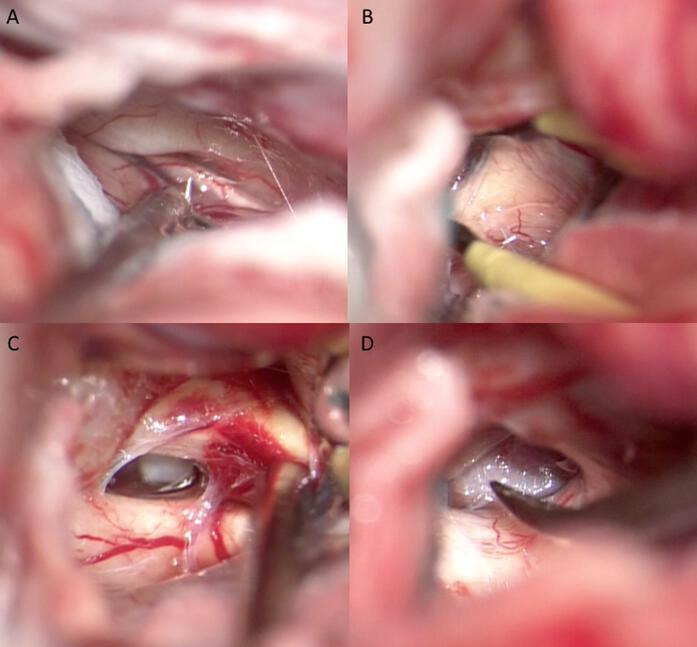
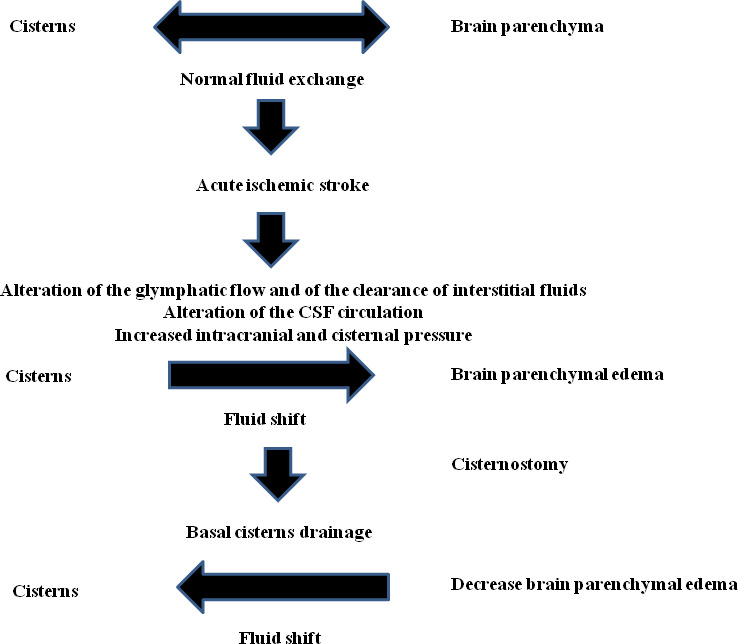
Background: The ischaemic stroke of the territory of the middle cerebral artery represents an event burdened by high mortality and severe morbidity. The proposed medical treatments do not always prove effective. Decompressive craniectomy allows the ischaemic tissue to shift through the surgical defect rather than to the unaffected regions of the brain, thus avoiding secondary damage due to increased intracranial pressure. In this study, we propose a novel treatment for these patients characterised by surgical fenestration of the cisterns of the skull base.
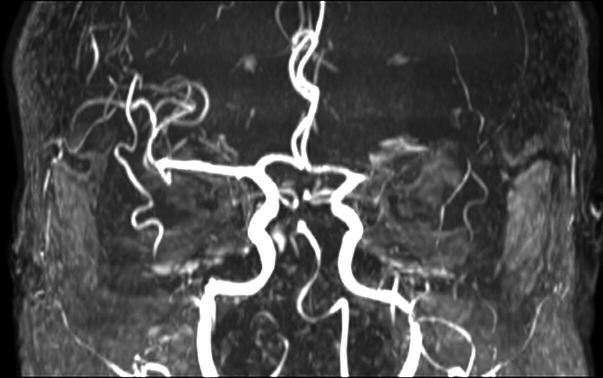
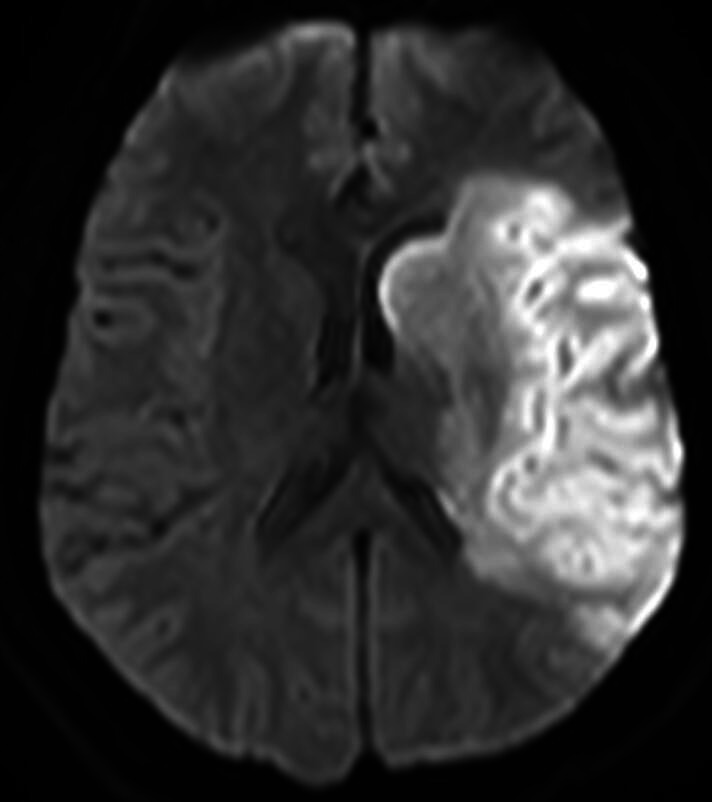
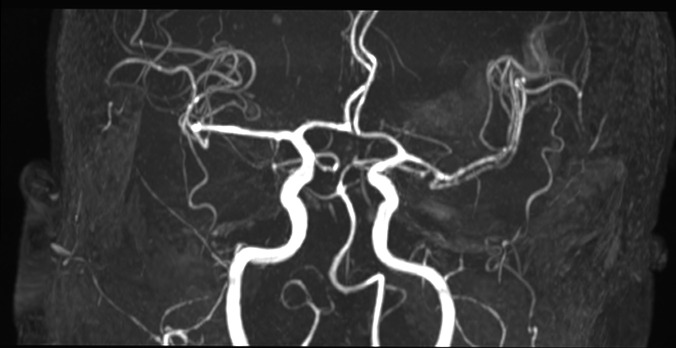
Methods: We have treated 16 patients affected by malignant middle cerebral artery ischaemia and treated with cisternostomy between August 2018 and December 2019. The clinical history, neurological examination findings and neuroradiological studies (brain CT, CT angiography, MRI) were performed to diagnose stroke. Clinical examination was recorded on admission and preoperatively using the Glasgow Coma Scale and the National Institutes of Health Stroke Scale.
Results: The study included 16 patients, 10 males and 6 females. The mean age at surgery was 60.1 years (range 19-73). Surgical procedure was performed in all patients. The patients underwent immediate postoperative CT scan and were in the early hours evaluated in sedation window. In total, we recorded two deaths (12.5%). A functional outcome between mRS 0-3, defined as favourable, was observed in 9 (64.2%) patients 9 months after discharge. A functional outcome between mRS 4-6, defined as poor, was observed in 5 (35.7%) patients 9 months after discharge.
Conclusions: The obtained clinical results appear, however, substantially overlapping to decompressive craniectomy. Cisternostomy results in a favourable functional outcome after 9 months. This proposed technique permits that the patient no longer should be undergone cranioplasty thus avoiding the possible complications related to this procedure. The results are certainly interesting but higher case numbers are needed to reach definitive conclusions.
Keywords: Intracranial Pressure; Magnetic Resonance Imaging; Stroke.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Decompressive hemicraniectomy for malignant middle cerebral artery infarction including patients with additional involvement of the anterior and/or posterior cerebral artery territory-outcome analysis and definition of prognostic factors.Acta Neurochir (Wien). 2018 Jan;160(1):83-89. doi: 10.1007/s00701-017-3329-3. Epub 2017 Sep 30. Acta Neurochir (Wien). 2018. PMID: 28965156
-
Nationwide survey of decompressive hemicraniectomy for malignant middle cerebral artery infarction in Japan.World Neurosurg. 2014 Dec;82(6):1158-63. doi: 10.1016/j.wneu.2014.07.015. Epub 2014 Jul 18. World Neurosurg. 2014. PMID: 25045787
-
10-Year Institutional Retrospective Case Series of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction (mMCAI).World Neurosurg. 2016 Dec;96:383-389. doi: 10.1016/j.wneu.2016.09.004. Epub 2016 Sep 14. World Neurosurg. 2016. PMID: 27639522
-
Reconsidering the role of decompressive craniectomy for neurological emergencies.J Crit Care. 2017 Jun;39:185-189. doi: 10.1016/j.jcrc.2017.03.006. Epub 2017 Mar 8. J Crit Care. 2017. PMID: 28285834 Review.
-
[Acute surgical treatment of malignant stroke].Ugeskr Laeger. 2016 Oct 24;178(43):V05160359. Ugeskr Laeger. 2016. PMID: 27808032 Review. Danish.
Cited by
-
Basic study on cryopreservation of rat calvarial osteoblasts with different cryoprotectants.Cell Tissue Bank. 2024 Sep;25(3):755-764. doi: 10.1007/s10561-024-10142-3. Epub 2024 Jul 8. Cell Tissue Bank. 2024. PMID: 38976150
-
The basal cisternostomy for management of severe traumatic brain injury: A retrospective study.Chin J Traumatol. 2025 Mar;28(2):118-123. doi: 10.1016/j.cjtee.2024.09.007. Epub 2024 Nov 20. Chin J Traumatol. 2025. PMID: 39632242 Free PMC article.
References
-
- Hacke W, Schwab S, Horn M. Middle cerebral infarction. Arch Neurol 1996;54:309–15. - PubMed
-
- Godoy D, Piñero G, Cruz-Flores S. Malignant hemispheric infarction of the middle cerebral artery. Diagnostic consideration. Neurología 2016;31:332–43. - PubMed
-
- Soinne L, Sundararajan S, Strbian D. Malignant hemispheric infarction: diagnosis and management by hemicraniectomy. Stroke 2014;45:185–7. - PubMed
-
- Elsayed A, Elsayed A. Decompressive craniectomy in malignant hemispheric infarction: favorable outcome and disability. Egypt J Neurol Psychiatry Neurosurg 2019;55:25. 10.1186/s41983-019-0077-8 - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical