

Improving intervention design to promote cervical cancer screening among hard-to-reach women: assessing beliefs and predicting individual attendance probabilities in Bogotá, Colombia
- PMID: 35672816
- PMCID: PMC9172610
- DOI: 10.1186/s12905-022-01800-3
Improving intervention design to promote cervical cancer screening among hard-to-reach women: assessing beliefs and predicting individual attendance probabilities in Bogotá, Colombia
Abstract
Background: Despite being a preventable disease, cervical cancer continues to be a public health concern, affecting mainly lower and middle-income countries. Therefore, in Bogotá a home-visit based program was instituted to increase screening uptake. However, around 40% of the visited women fail to attend their Pap smear test appointments. Using this program as a case study, this paper presents a methodology that combines machine learning methods, using routinely collected administrative data, with Champion's Health Belief Model to assess women's beliefs about cervical cancer screening. The aim is to improve the cost-effectiveness of behavioural interventions aiming to increase attendance for screening. The results presented here relate specifically to the case study, but the methodology is generic and can be applied in all low-income settings.
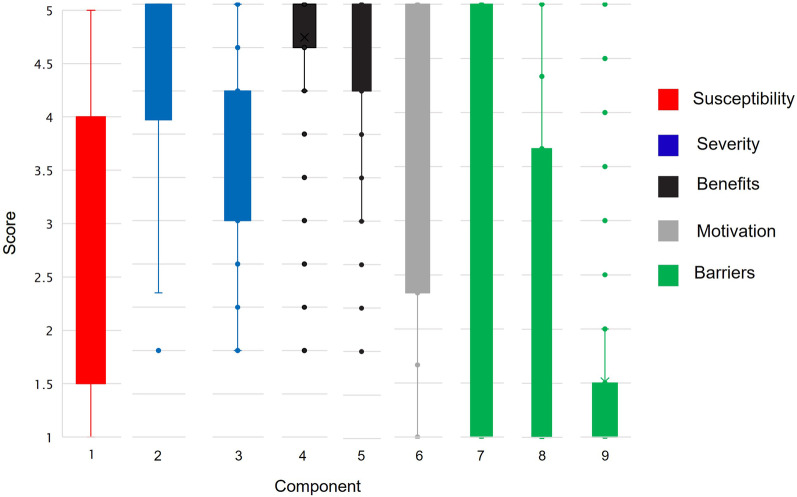
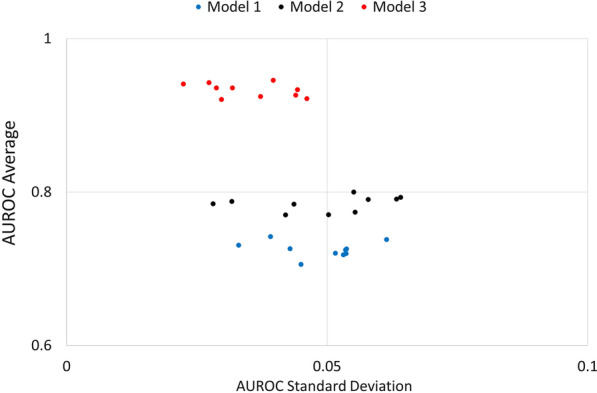
Methods: This is a cross-sectional study using two different datasets from the same population and a sequential modelling approach. To assess beliefs, we used a 37-item questionnaire to measure the constructs of the CHBM towards cervical cancer screening. Data were collected through a face-to-face survey (N = 1699). We examined instrument reliability using Cronbach's coefficient and performed a principal component analysis to assess construct validity. Then, Kruskal-Wallis and Dunn tests were conducted to analyse differences on the HBM scores, among patients with different poverty levels. Next, we used data retrieved from administrative health records (N = 23,370) to fit a LASSO regression model to predict individual no-show probabilities. Finally, we used the results of the CHBM in the LASSO model to improve its accuracy.
Results: Nine components were identified accounting for 57.7% of the variability of our data. Lower income patients were found to have a lower Health motivation score (p-value < 0.001), a higher Severity score (p-value < 0.001) and a higher Barriers score (p-value < 0.001). Additionally, patients between 25 and 30 years old and with higher poverty levels are less likely to attend their appointments (O.R 0.93 (CI: 0.83-0.98) and 0.74 (CI: 0.66-0.85), respectively). We also found a relationship between the CHBM scores and the patient attendance probability. Average AUROC score for our prediction model is 0.9.
Conclusion: In the case of Bogotá, our results highlight the need to develop education campaigns to address misconceptions about the disease mortality and treatment (aiming at decreasing perceived severity), particularly among younger patients living in extreme poverty. Additionally, it is important to conduct an economic evaluation of screening options to strengthen the cervical cancer screening program (to reduce perceived barriers). More widely, our prediction approach has the potential to improve the cost-effectiveness of behavioural interventions to increase attendance for screening in developing countries where funding is limited.
Keywords: Cervical cancer screening; Hard-to-reach women; Health belief model; No-show prediction.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Understanding no-show behaviour for cervical cancer screening appointments among hard-to-reach women in Bogotá, Colombia: A mixed-methods approach.PLoS One. 2022 Jul 22;17(7):e0271874. doi: 10.1371/journal.pone.0271874. eCollection 2022. PLoS One. 2022. PMID: 35867727 Free PMC article.
-
Factors associated with the intention to undergo Pap smear testing in the rural areas of Indonesia: a health belief model.Reprod Health. 2021 Jun 30;18(1):138. doi: 10.1186/s12978-021-01188-7. Reprod Health. 2021. PMID: 34193195 Free PMC article.
-
Beliefs and perceptions regarding cervical cancer and screening associated with Pap smear uptake in Johannesburg: A cross-sectional study.PLoS One. 2021 Feb 10;16(2):e0246574. doi: 10.1371/journal.pone.0246574. eCollection 2021. PLoS One. 2021. PMID: 33566798 Free PMC article.
-
Barriers to uptake of cervical cancer screening services in low-and-middle-income countries: a systematic review.BMC Womens Health. 2022 Dec 2;22(1):486. doi: 10.1186/s12905-022-02043-y. BMC Womens Health. 2022. PMID: 36461001 Free PMC article.
-
Low-Cost Interventions to Improve Cervical Cancer Screening: An Integrative Review.Oncol Nurs Forum. 2022 Dec 16;50(1):59-78. doi: 10.1188/23.ONF.59-78. Oncol Nurs Forum. 2022. PMID: 37677791 Review.
Cited by
-
Accurate deep learning model using semi-supervised learning and Noisy Student for cervical cancer screening in low magnification images.PLoS One. 2023 May 18;18(5):e0285996. doi: 10.1371/journal.pone.0285996. eCollection 2023. PLoS One. 2023. PMID: 37200281 Free PMC article.
-
Impact of virtual education based on health belief model on cervical cancer screening behavior in middle-aged women: A quasi-experimental study.Cancer Rep (Hoboken). 2024 Apr;7(4):e2058. doi: 10.1002/cnr2.2058. Cancer Rep (Hoboken). 2024. PMID: 38600048 Free PMC article.
References
-
- Tatari CR, Andersen B, Andersen B, Brogaard T, Badre-Esfahani SK, Badre-Esfahani SK, et al. Perceptions about cancer and barriers towards cancer screening among ethnic minority women in a deprived area in Denmark - a qualitative study. BMC Public Health. 2020;20:1–10. doi: 10.1186/s12889-020-09037-1. - DOI - PMC - PubMed
