

Does the addition of whole-body MRI to routine imaging influence real-world treatment decisions in metastatic breast cancer?
- PMID: 35672838
- PMCID: PMC9172188
- DOI: 10.1186/s40644-022-00464-4
Does the addition of whole-body MRI to routine imaging influence real-world treatment decisions in metastatic breast cancer?
Abstract
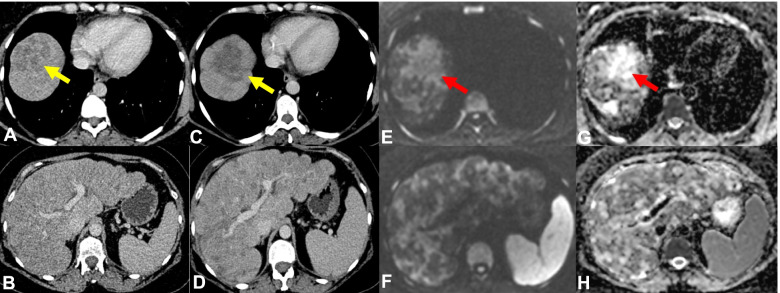
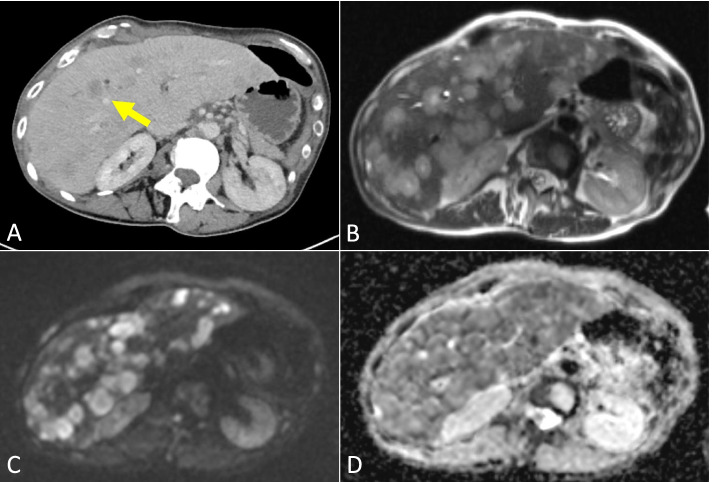
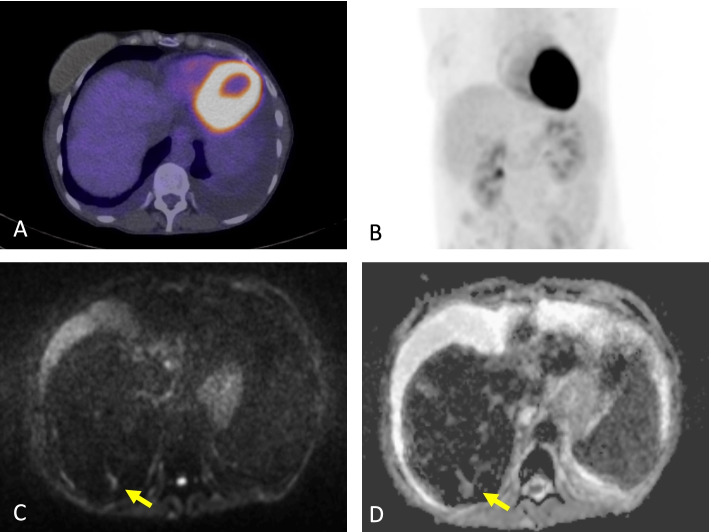
Background: The assessment of metastatic breast cancer (MBC) can be limited with routine imaging such as computed tomography (CT) especially in bone-only or bone-predominant disease. This analysis investigates the effects of the use of WBMRI in addition to the use of routine CT, bone scintigraphy (BS) and fluorine-18-fluorodeoxyglucose positron emission tomography with computed tomography (FDG-PET/CT) on influencing systemic anti-cancer treatment (SACT) decisions in patients with known MBC.
Methods: MBC patients undergoing SACT who had WBMRI undertaken within 8 weeks of either a routine CT, BS or FDG-PET/CT were reviewed retrospectively. The clinical indications for undertaking the WBMRI examinations were recorded. Data on the extent and distribution of the disease were collected and discordance/concordance of disease status across the imaging modalities were compared. SACT decisions at each time point were also evaluated.
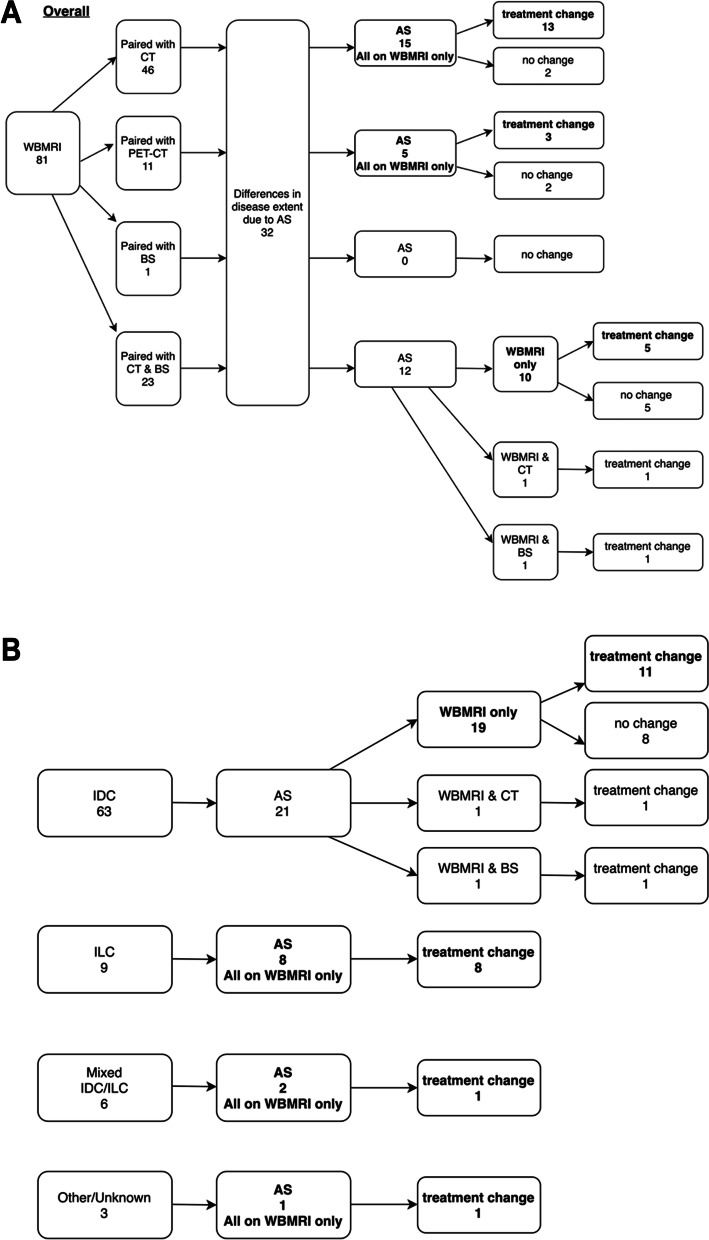
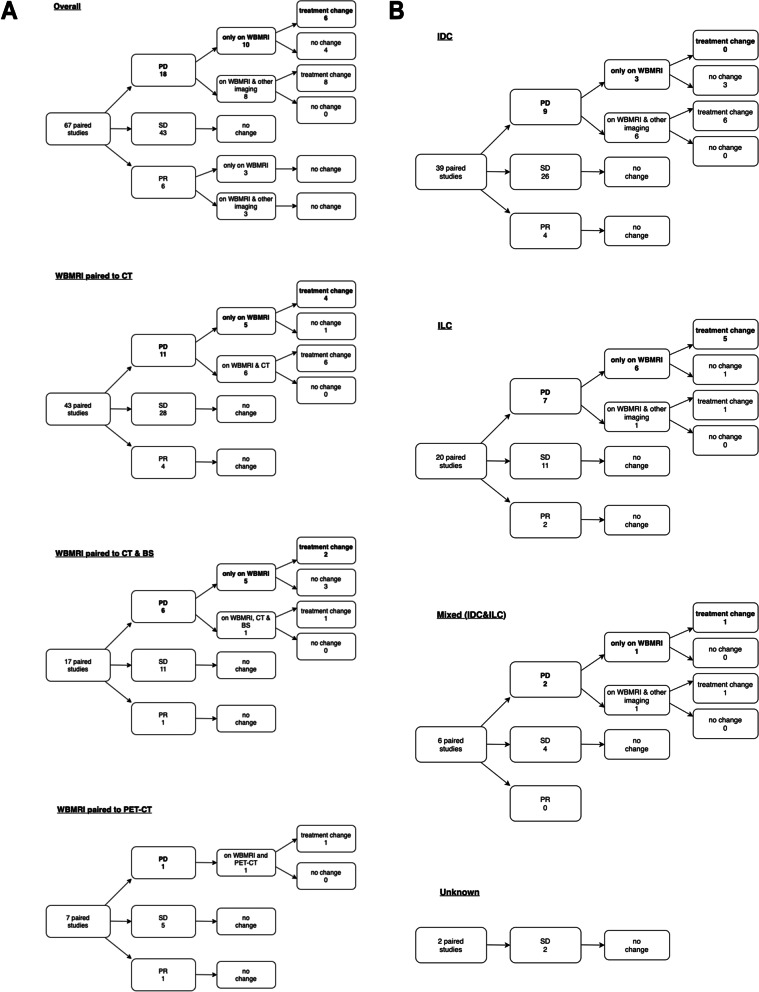
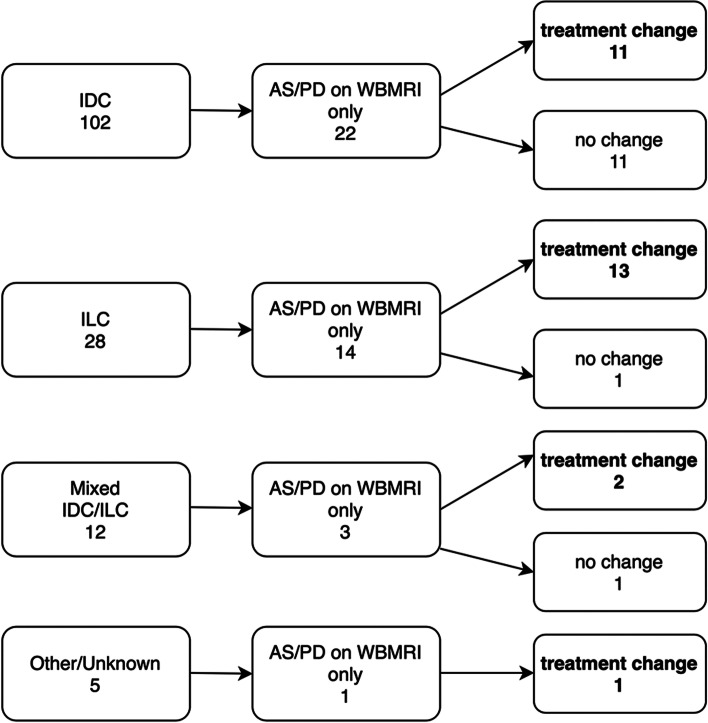
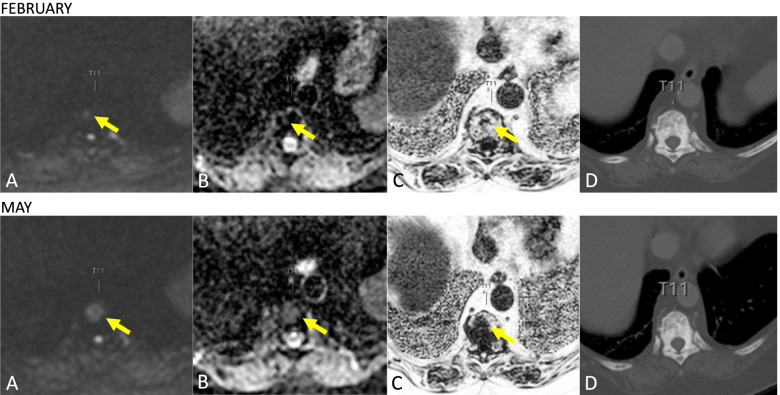
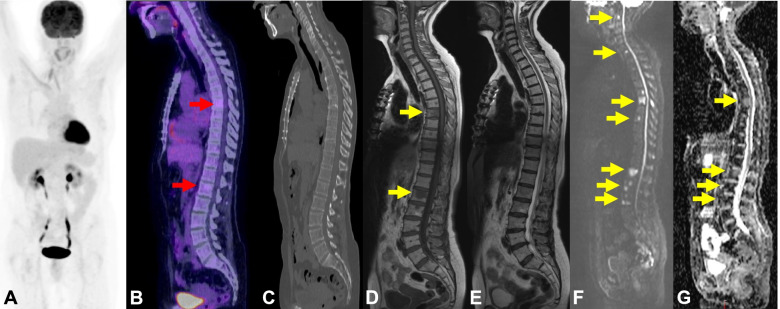
Results: There were 105 MBC patients with 148 WBMRI studies paired with CT, BS or FDG-PET/CT. 50 pairs (33.8%) showed differences in the extent of disease, with 44 pairs due to additional sites (AS) reported on WBMRI alone. 81 patients (Group 1) had one WBMRI paired with routine imaging due to a variety of indications, with clinical symptoms (such as bone pain) being the most common (24.7%). 24 patients (Group 2) had more than one WBMRI study paired with routine imaging comprising 67 pairs. 13/67 pairs (19.4%) showed discordance in assessments. 10/13 pairs had progressive disease (PD) reported on WBMRI alone. SACT change due to AS reported on WBMRI alone occurred in 21/23 pairs (91.3%) in Group 1. SACT change due to PD reported on WBMRI alone in Group 2 occurred in 6/14 pairs (42.9%). SACT change due to AS/PD in both groups occurred in 11/102 pairs (10.8%) with known invasive ductal carcinoma (IDC) and 13/28 pairs (46.4%) with invasive lobular carcinoma (ILC).
Conclusions: The use of WBMRI in MBC led to earlier recognition of PD and SACT change compared with the other imaging modalities. A higher proportion of discordant response assessments and SACT changes were observed in ILC compared with IDC in our patient group, although larger-scale studies are required to investigate this further.
Keywords: Cancer treatment; Diffusion-weighted imaging; Metastatic breast cancer; Response assessment; Whole-body magnetic resonance imaging.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- The Royal College of Radiologists. Guidance on screening and symptomatic breast imaging: Fourth edition. Clinical Radiology The Royal College of Radiologists [Internet]. The Royal College of Radiologists; 2019 [cited 2021 May 9]; Available from: www.rcr.ac.uk
-
- Gradishar WJ, Moran MS, Abraham J, Aft R, Agnese D, Allison KH, et al. NCCN Guidelines® insights: breast cancer, Version 4.2021. J Natl Comprehens Cancer Netw. 2021;19(484):93. - PubMed
-
- Coleman RE. Clinical Features of Metastatic Bone Disease and Risk of Skeletal Morbidity. Clin Cancer Res. 2006;12(6243s LP):6249s. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
