

Worsening or improving hypoalbuminemia during continuous renal replacement therapy is predictive of patient outcome: a single-center retrospective study
- PMID: 35672868
- PMCID: PMC9171968
- DOI: 10.1186/s40560-022-00620-9
Worsening or improving hypoalbuminemia during continuous renal replacement therapy is predictive of patient outcome: a single-center retrospective study
Abstract
Background: Hypoalbuminemia at the initiation of continuous renal replacement therapy (CRRT) is a risk factor for poor patient outcomes. However, it is unknown whether the patterns of changes in serum albumin levels during CRRT can be used to predict patient outcomes.
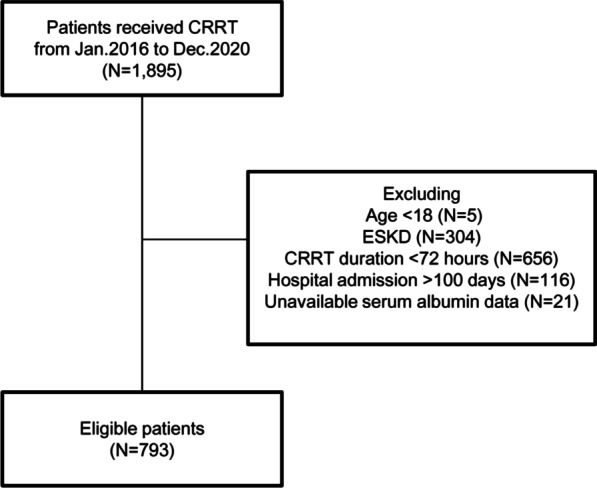
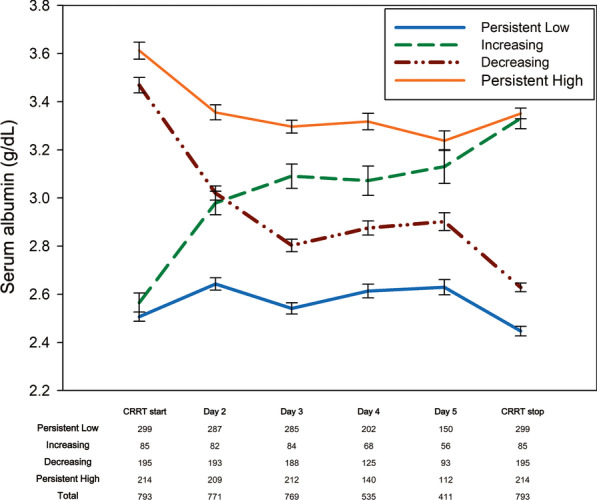
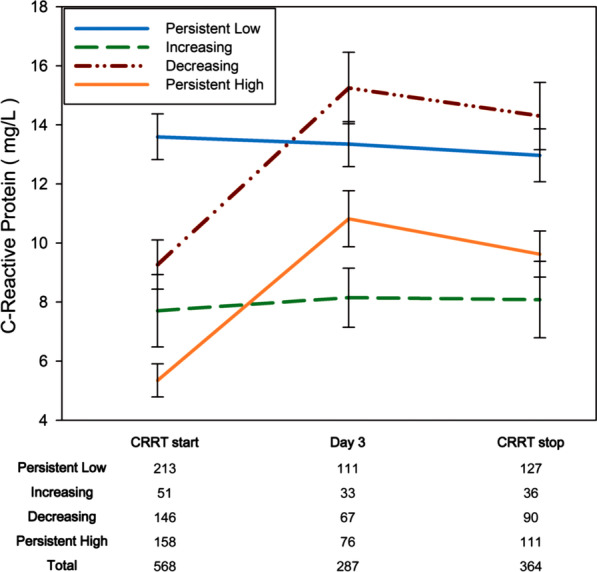
Methods: This retrospective study analyzed data that had been consecutively collected from January 2016 to December 2020 at the Third Affiliated Hospital. We included patients with acute kidney injury who received CRRT for ≥ 72 h. We divided the patients into four groups based on their serum albumin levels (albumin ≥ 3.0 g/dL or < 3.0 g/dL) at the initiation and termination of CRRT.
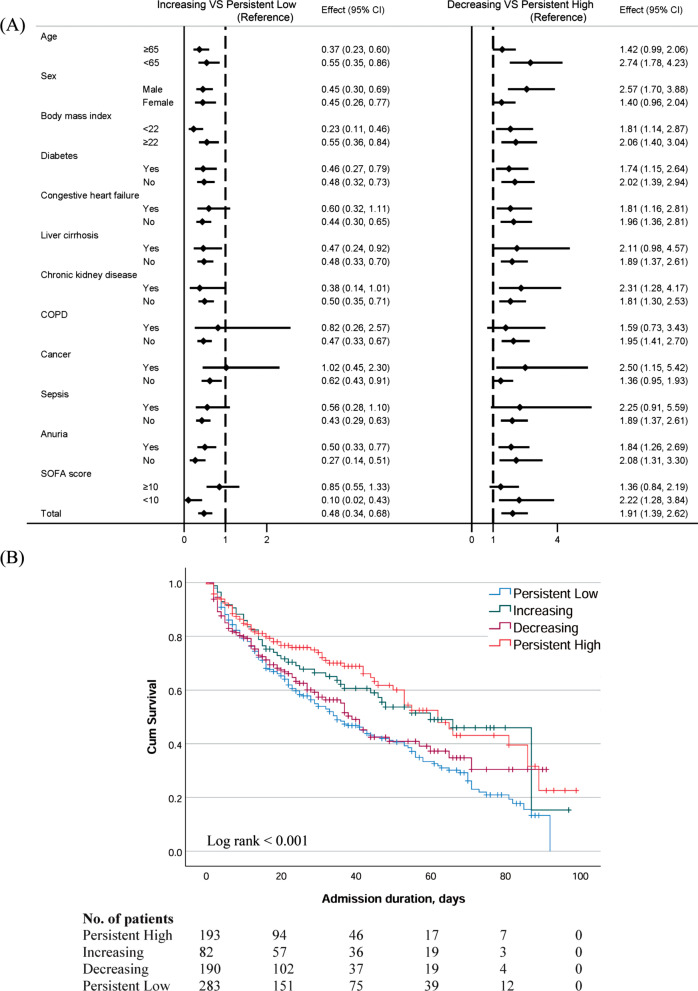
Results: The 793 patients in this study were categorized into the following albumin groups: persistently low, 299 patients (37.7%); increasing, 85 patients (10.4%); decreasing, 195 patients (24.6%); and persistently high, 214 patients (27.1%). In-hospital mortality rates were highest in the persistently low and decreasing groups, followed by the increasing and persistently high groups. The hazard ratio for in-hospital mortality was 0.481 (0.340-0.680) in the increasing group compared to the persistently low group; it was 1.911 (1.394-2.620) in the decreasing group compared to the persistently high group. The length of ICU stay was 3.55 days longer in the persistently low group than in the persistently high group.
Conclusions: Serum albumin levels changed during CRRT, and monitoring of patterns of change in serum albumin levels is useful for predicting in-hospital mortality and the length of ICU stay.
Keywords: Acute kidney injury; Albumin; Continuous renal replacement therapy; Hypoalbuminemia.
© 2022. The Author(s).
Conflict of interest statement
None of the authors has any potential conflict of interest.
Figures
Similar articles
-
Impact of hypoalbuminemia on mortality in critically ill patients requiring continuous renal replacement therapy.J Crit Care. 2022 Apr;68:72-75. doi: 10.1016/j.jcrc.2021.12.008. Epub 2021 Dec 17. J Crit Care. 2022. PMID: 34929529
-
Association of hypoalbuminemia with short-term and long-term mortality in patients undergoing continuous renal replacement therapy.Kidney Res Clin Pract. 2020 Mar 31;39(1):47-53. doi: 10.23876/j.krcp.19.088. Kidney Res Clin Pract. 2020. PMID: 31995708 Free PMC article.
-
[Relationship between the timing of initiation of continuous renal replacement therapy and the prognosis of patients with sepsis-associated acute kidney injury].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Nov;32(11):1352-1355. doi: 10.3760/cma.j.cn121430-20200304-00206. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 33463496 Chinese.
-
The role of the specialized team in the operation of continuous renal replacement therapy: a single-center experience.BMC Nephrol. 2017 Nov 13;18(1):332. doi: 10.1186/s12882-017-0746-8. BMC Nephrol. 2017. PMID: 29132321 Free PMC article.
-
Predictors of Hypophosphatemia and Outcomes during Continuous Renal Replacement Therapy.Blood Purif. 2020;49(6):700-707. doi: 10.1159/000507421. Epub 2020 Apr 22. Blood Purif. 2020. PMID: 32320987
Cited by
-
A Clinical Nomogram for Predicting Substandard Serum Valproic Acid Concentrations in Chinese Patients With Epilepsy.Curr Ther Res Clin Exp. 2024 Dec 26;102:100771. doi: 10.1016/j.curtheres.2024.100771. eCollection 2025. Curr Ther Res Clin Exp. 2024. PMID: 39895998 Free PMC article.
-
The association between albumin corrected anion gap and ICU mortality in acute kidney injury patients requiring continuous renal replacement therapy.Intern Emerg Med. 2022 Nov;17(8):2315-2322. doi: 10.1007/s11739-022-03093-8. Epub 2022 Sep 16. Intern Emerg Med. 2022. PMID: 36112320 Free PMC article.
-
The Impact of Hypoalbuminemia on Inflammatory Markers, Serum Creatinine, Hemoglobin and Outcome in Critically ill Patients With COVID-19 Infection-Retrospective Observation Study.Acta Inform Med. 2025;33(2):96-100. doi: 10.5455/aim.2025.33.96-100. Acta Inform Med. 2025. PMID: 40606241 Free PMC article.
-
Association between hypoalbuminemia and mortality in patients undergoing continuous renal replacement therapy: A systematic review and meta-analysis.PLoS One. 2023 Mar 30;18(3):e0283623. doi: 10.1371/journal.pone.0283623. eCollection 2023. PLoS One. 2023. PMID: 36996133 Free PMC article.
-
Advanced lung cancer inflammation index is associated with mortality in critically ill patients with non-traumatic cerebral hemorrhage.Sci Rep. 2025 Apr 29;15(1):14972. doi: 10.1038/s41598-025-98854-8. Sci Rep. 2025. PMID: 40301437 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
