

2022 Guidelines of the Taiwan Society of Cardiology and the Taiwan Hypertension Society for the Management of Hypertension
- PMID: 35673334
- PMCID: PMC9121756
- DOI: 10.6515/ACS.202205_38(3).20220321A
2022 Guidelines of the Taiwan Society of Cardiology and the Taiwan Hypertension Society for the Management of Hypertension
Abstract
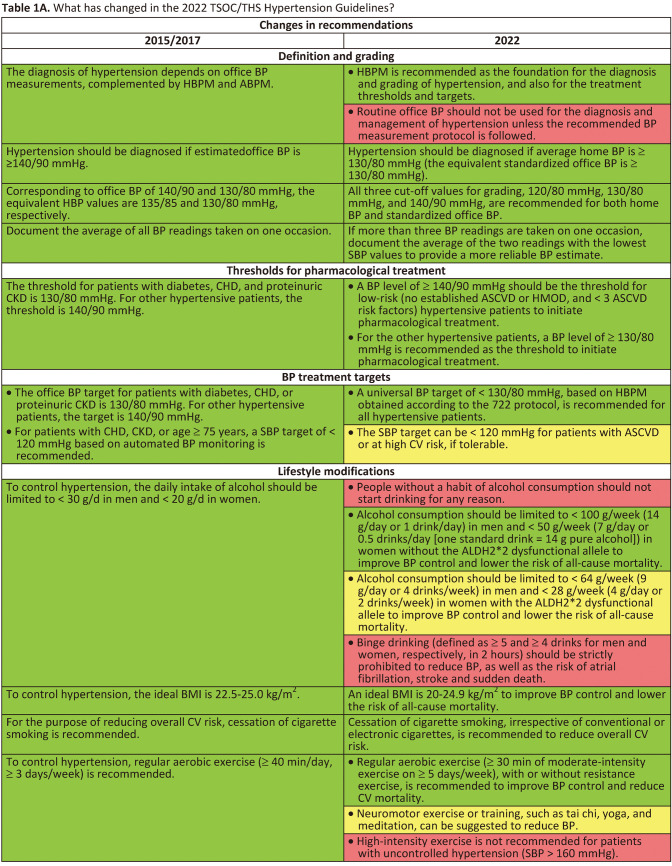
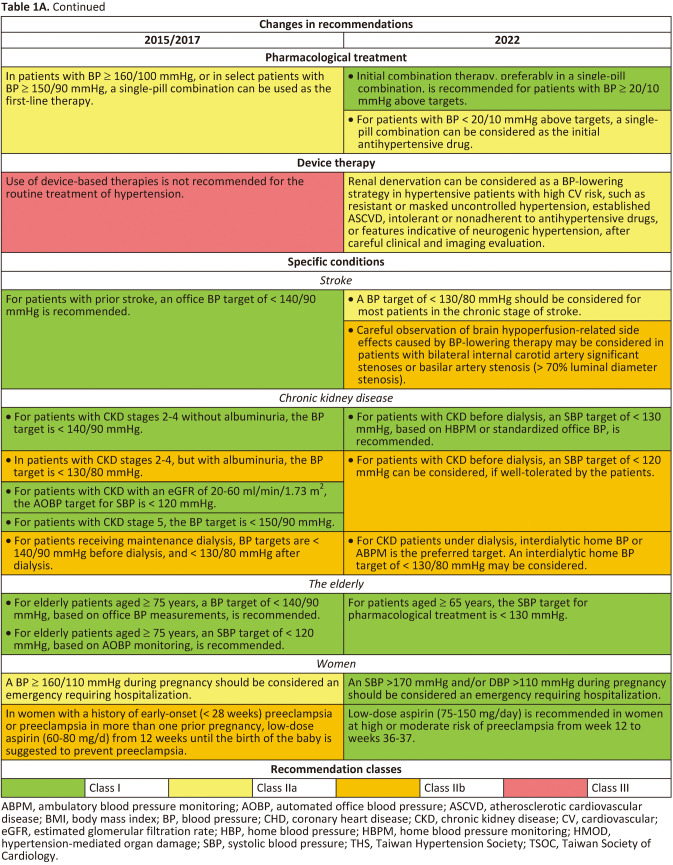
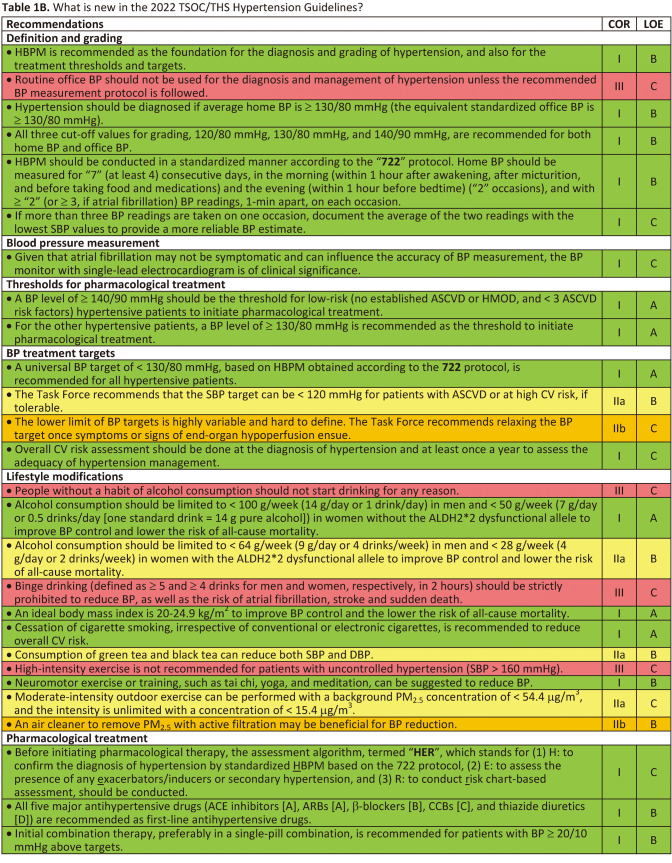
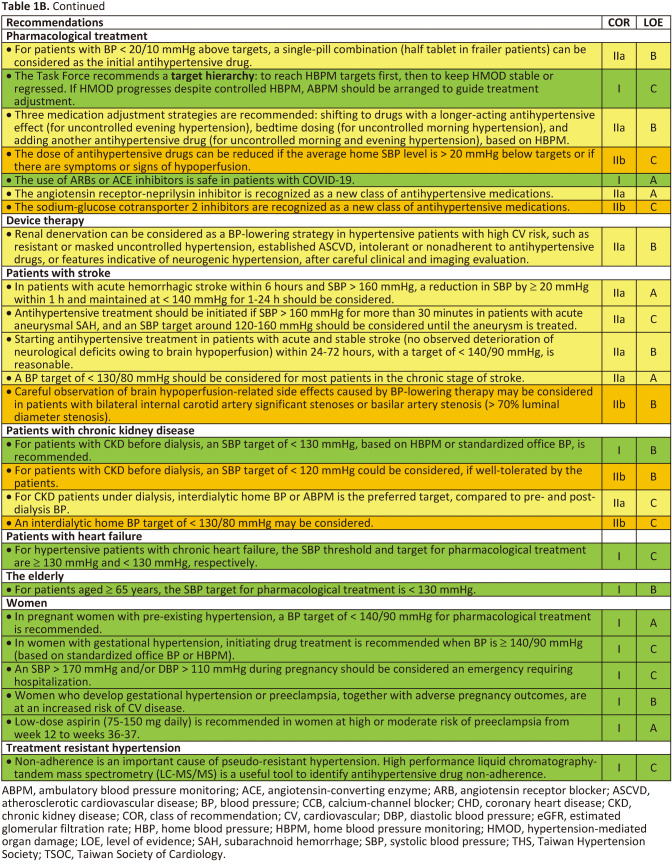
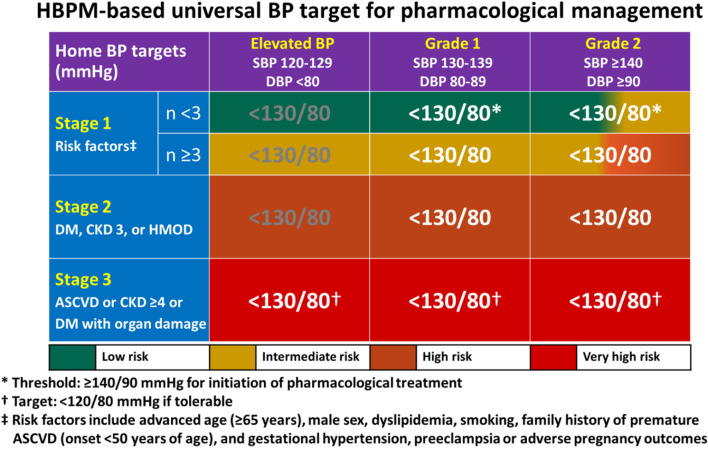
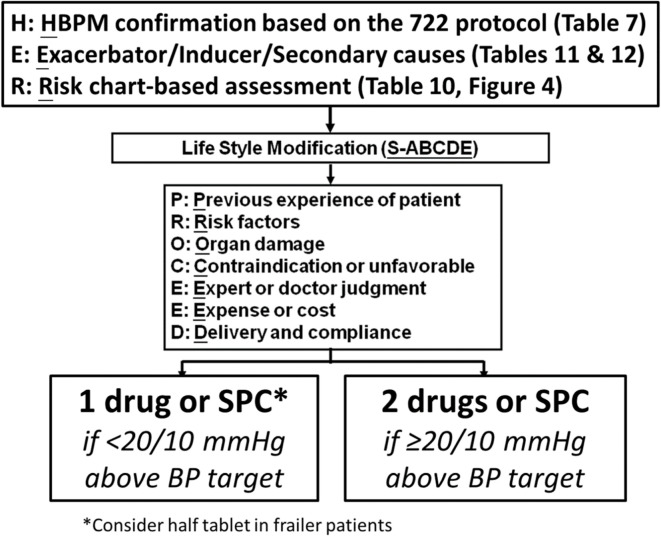
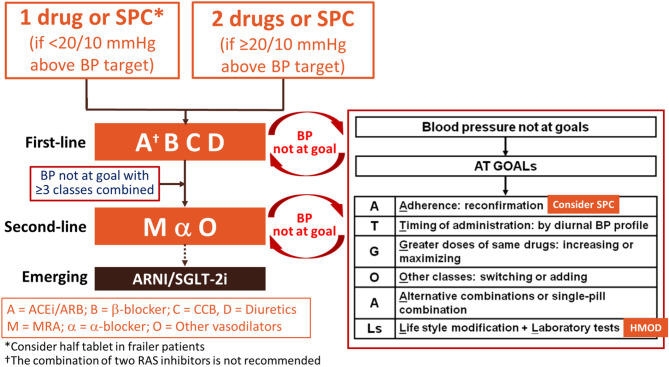
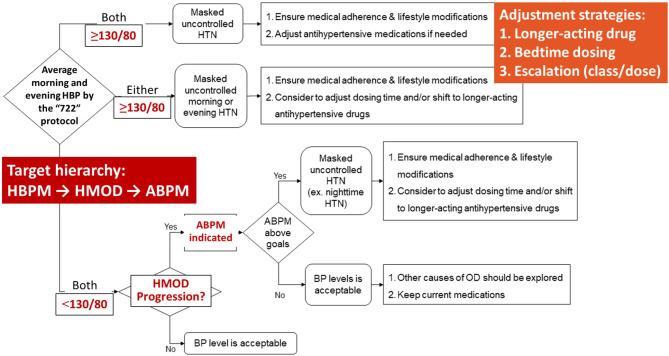
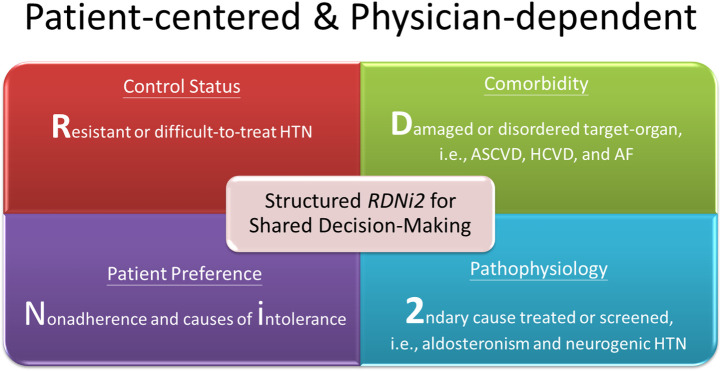
Hypertension is the most important modifiable cause of cardiovascular (CV) disease and all-cause mortality worldwide. Despite the positive correlations between blood pressure (BP) levels and later CV events since BP levels as low as 100/60 mmHg have been reported in numerous epidemiological studies, the diagnostic criteria of hypertension and BP thresholds and targets of antihypertensive therapy have largely remained at the level of 140/90 mmHg in the past 30 years. The publication of both the SPRINT and STEP trials (comprising > 8,500 Caucasian/African and Chinese participants, respectively) provided evidence to shake this 140/90 mmHg dogma. Another dogma regarding hypertension management is the dependence on office (or clinic) BP measurements. Although standardized office BP measurements have been widely recommended and adopted in large-scale CV outcome trials, the practice of office BP measurements has never been ideal in real-world practice. Home BP monitoring (HBPM) is easy to perform, more likely to be free of environmental and/or emotional stress, feasible to document long-term BP variations, of good reproducibility and reliability, and more correlated with hypertension-mediated organ damage (HMOD) and CV events, compared to routine office BP measurements. In the 2022 Taiwan Hypertension Guidelines of the Taiwan Society of Cardiology (TSOC) and the Taiwan Hypertension Society (THS), we break these two dogmas by recommending the definition of hypertension as ≥ 130/80 mmHg and a universal BP target of < 130/80 mmHg, based on standardized HBPM obtained according to the 722 protocol. The 722 protocol refers to duplicate BP readings taken per occasion ("2"), twice daily ("2"), over seven consecutive days ("7"). To facilitate implementation of the guidelines, a series of flowcharts encompassing assessment, adjustment, and HBPM-guided hypertension management are provided. Other key messages include that: 1) lifestyle modification, summarized as the mnemonic S-ABCDE, should be applied to people with elevated BP and hypertensive patients to reduce life-time BP burden; 2) all 5 major antihypertensive drugs (angiotensin-converting enzyme inhibitors [A], angiotensin receptor blockers [A], β-blockers [B], calcium-channel blockers [C], and thiazide diuretics [D]) are recommended as first-line antihypertensive drugs; 3) initial combination therapy, preferably in a single-pill combination, is recommended for patients with BP ≥ 20/10 mmHg above targets; 4) a target hierarchy (HBPM-HMOD- ambulatory BP monitoring [ABPM]) should be considered to optimize hypertension management, which indicates reaching the HBPM target first and then keeping HMOD stable or regressed, otherwise ABPM can be arranged to guide treatment adjustment; and 5) renal denervation can be considered as an alternative BP-lowering strategy after careful clinical and imaging evaluation.
Keywords: Blood pressure; Diagnosis; Drug; Guidelines; Hypertension; Treatment.
Figures
References
-
- Choi YJ, Kim SH, Kang SH, et al. Reconsidering the cut-off diastolic blood pressure for predicting cardiovascular events: a nationwide population-based study from Korea. Eur Heart J. 2019;40:724–731. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous