

Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antibody lateral flow assay for antibody prevalence studies following vaccination: a diagnostic accuracy study
- PMID: 35673545
- PMCID: PMC9152464
- DOI: 10.12688/wellcomeopenres.17231.2
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antibody lateral flow assay for antibody prevalence studies following vaccination: a diagnostic accuracy study
Abstract
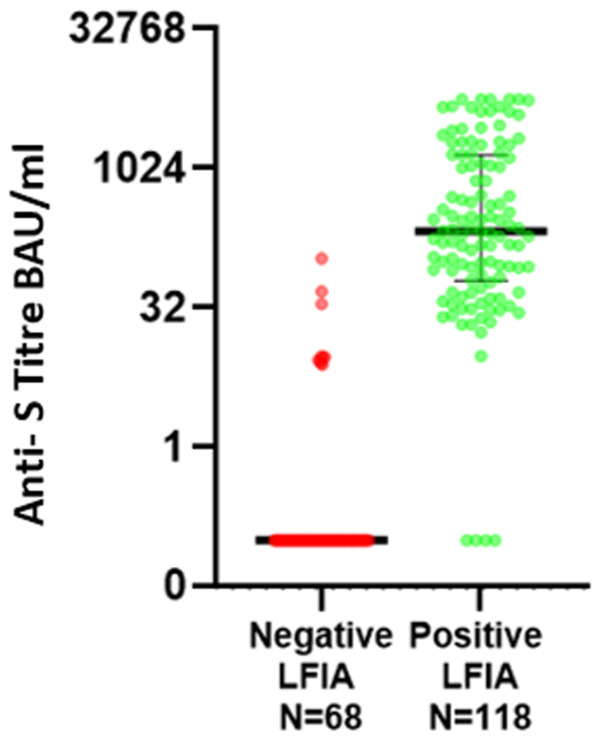
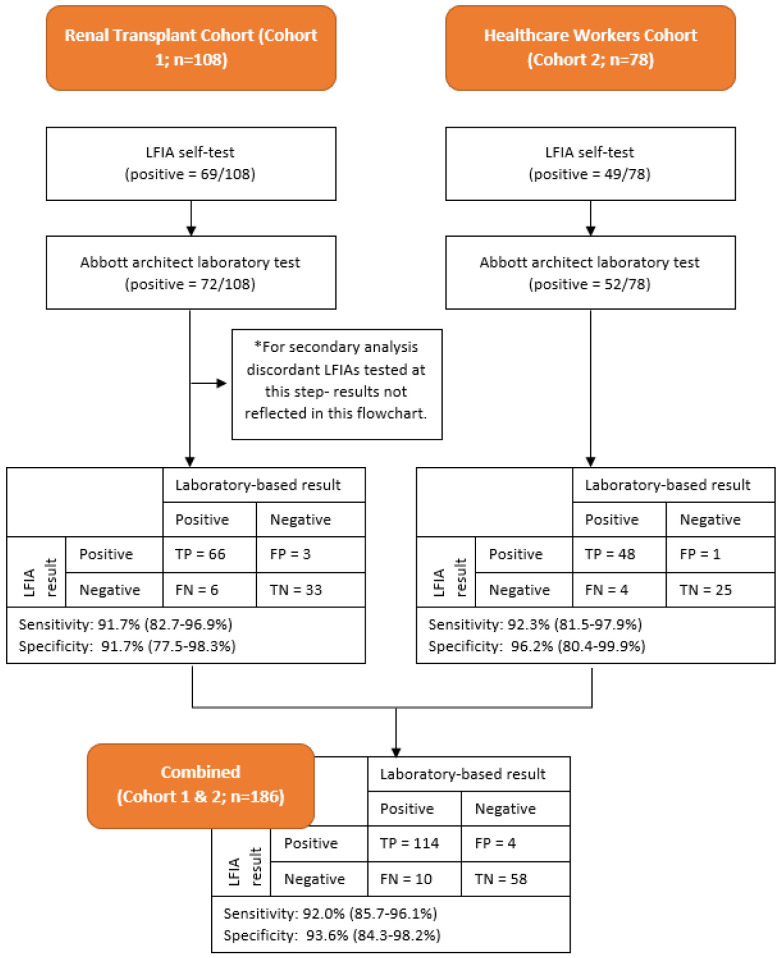
Background: Lateral flow immunoassays (LFIAs) are able to achieve affordable, large scale antibody testing and provide rapid results without the support of central laboratories. As part of the development of the REACT programme extensive evaluation of LFIA performance was undertaken with individuals following natural infection. Here we assess the performance of the selected LFIA to detect antibody responses in individuals who have received at least one dose of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccine. Methods: This was a prospective diagnostic accuracy study. Sampling was carried out at renal outpatient clinic and healthcare worker testing sites at Imperial College London NHS Trust. Two cohorts of patients were recruited; the first was a cohort of 108 renal transplant patients attending clinic following two doses of SARS-CoV-2 vaccine, the second cohort comprised 40 healthcare workers attending for first SARS-CoV-2 vaccination and subsequent follow up. During the participants visit, finger-prick blood samples were analysed on LFIA device, while paired venous sampling was sent for serological assessment of antibodies to the spike protein (anti-S) antibodies. Anti-S IgG was detected using the Abbott Architect SARS-CoV-2 IgG Quant II CMIA. A total of 186 paired samples were collected. The accuracy of Fortress LFIA in detecting IgG antibodies to SARS-CoV-2 compared to anti-spike protein detection on Abbott Assay Results: The LFIA had an estimated sensitivity of 92.0% (114/124; 95% confidence interval [CI] 85.7% to 96.1%) and specificity of 93.6% (58/62; 95% CI 84.3% to 98.2%) using the Abbott assay as reference standard (using the threshold for positivity of 7.10 BAU/ml) Conclusions: Fortress LFIA performs well in the detection of antibody responses for intended purpose of population level surveillance but does not meet criteria for individual testing.
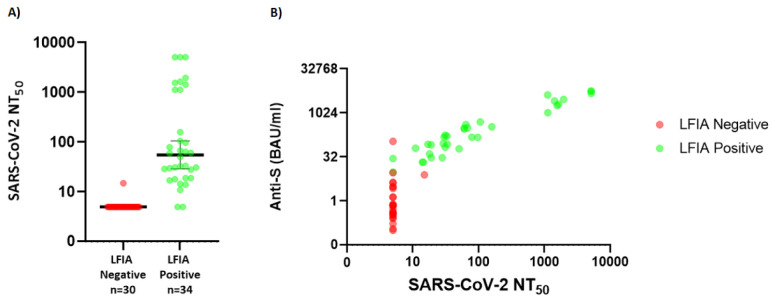
Keywords: Antibodies; Covid-19; LFIA; Lateral flow; Neutralisation; SARS-CoV-2; Seroprevalence.
Copyright: © 2022 Cann A et al.
Conflict of interest statement
No competing interests were disclosed.
Figures
References
-
- Ward H, Atchison C, Whitaker M, et al. : Antibody prevalence for SARS-CoV-2 following the peak of the pandemic in England: REACT2 study in 100,000 adults. bioRxiv. 2020. 10.1101/2020.08.12.20173690 - DOI
-
- Ward H, Cooke G, Atchison C, et al. : Declining prevalence of antibody positivity to SARS-CoV-2: a community study of 365,000 adults.Cold Spring Harbor Laboratory. medrxiv. 2020. 10.1101/2020.10.26.20219725 - DOI
-
- Ward H, Cooke G, Whitaker M, et al. : REACT-2 Round 5: increasing prevalence of SARS-CoV-2 antibodies demonstrate impact of the second wave and of vaccine roll-out in England.Cold Spring Harbor Laboratory. medrxiv. 2021. 10.1101/2021.02.26.21252512 - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
