

Comparative Effectiveness of Regimens for Drug-Susceptible Tuberculous Meningitis in Children and Adolescents: A Systematic Review and Aggregate-Level Data Meta-Analysis
- PMID: 35673608
- PMCID: PMC9167638
- DOI: 10.1093/ofid/ofac108
Comparative Effectiveness of Regimens for Drug-Susceptible Tuberculous Meningitis in Children and Adolescents: A Systematic Review and Aggregate-Level Data Meta-Analysis
Abstract
Background: Before August 2021, the only regimen recommended by the World Health Organization (WHO) to treat pediatric drug-susceptible tuberculous meningitis was a 12-month regimen consisting of isoniazid, rifampicin, ethambutol, and pyrazinamide (2HRZE/10HR). The comparative effectiveness of shorter regimens is unknown.
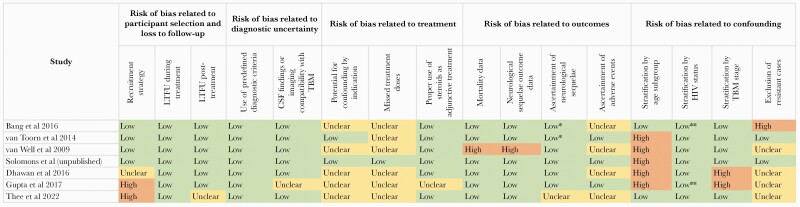
Methods: To inform a WHO guideline update, we undertook a systematic review and meta-analysis to evaluate outcomes from regimens of 6- to less than 12-months' duration that included, at a minimum, isoniazid, rifampicin, and pyrazinamide. We included studies that applied rigorous diagnostic criteria and reported outcomes for ≥10 children or adolescents. Using generalized linear mixed models, we estimated the random effects pooled proportions of patients with key outcomes.
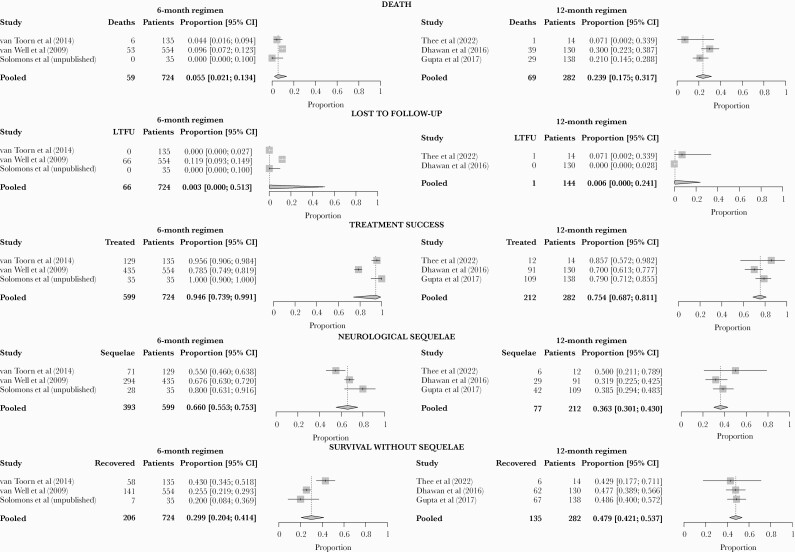
Results: Of 7 included studies, none compared regimens head-to-head. Three studies (724 patients) used a 6-month intensive regimen, which includes isoniazid and rifampicin at higher doses, pyrazinamide, and ethionamide instead of ethambutol (6HRZEto). Outcomes for this versus the 12-month regimen (282 patients, 3 studies) were, respectively, as follows: death, 5.5% (95% confidence interval [CI], 2.1%-13.4%) vs 23.9% (95% CI, 17.5%-31.7%); treatment success (survival with or without sequelae), 94.6% (95% CI, 73.9%-99.1%) vs 75.4% (95% CI, 68.7%-81.1%); and neurological sequelae among survivors, 66.0% (95% CI, 55.3%-75.3%) vs 36.3% (95% CI, 30.1%-43.0%). Relapse did not occur among 148 patients followed-up for 2 years after completing the 6-month intensive regimen.
Conclusions: Our findings are limited by the small number of studies and substantial potential for confounding. Nonetheless, the 6HRZEto regimen was associated with high treatment success and is now recommended by WHO as an alternative to the 12-month regimen.
Keywords: World Health Organization guidelines; neurological sequelae; treatment outcomes; tuberculosis.
© The Author(s) 2022.. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Chiang SS, Khan FA, Milstein MB, et al. Treatment outcomes of childhood tuberculous meningitis: a systematic review and meta-analysis. Lancet Infect Dis 2014; 14:947–57. - PubMed
-
- World Health Organization (WHO). Guidance for national tuberculosis programmes on the management of tuberculosis in children (2nd edition). Geneva, Switzerland: Global Tuberculosis Programme, World Health Organization (WHO). Available at: http://apps.who.int/iris/bitstream/handle/10665/112360/9789241548748_eng.... Accessed 26 January 2022.
-
- World Health Organization. Rapid Communication on Updated Guidance on the Management of Tuberculosis in Children and Adolescents. Geneva: World Health Organization; 2021.
-
- Guidelines for the Management of Tuberculosis in Children. Pretoria, South Africa: Department of Health; 2013.
-
- Kimberlin DW, Barnett ED, Lynfield R, Sawyer MH.. Tuberculosis. Red Book 2021: Report of the Committee on Infectious Diseases. Itasca, IL: American Academy of Pediatrics; 2021: pp 786–814.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
