

Prognostic factors following resection of intracranial metastases
- PMID: 35673669
- PMCID: PMC9168344
- DOI: 10.25259/SNI_103_2022
Prognostic factors following resection of intracranial metastases
Abstract
Background: The aim of this study was to identify prognostic factors associated with resection of intracranial metastases.
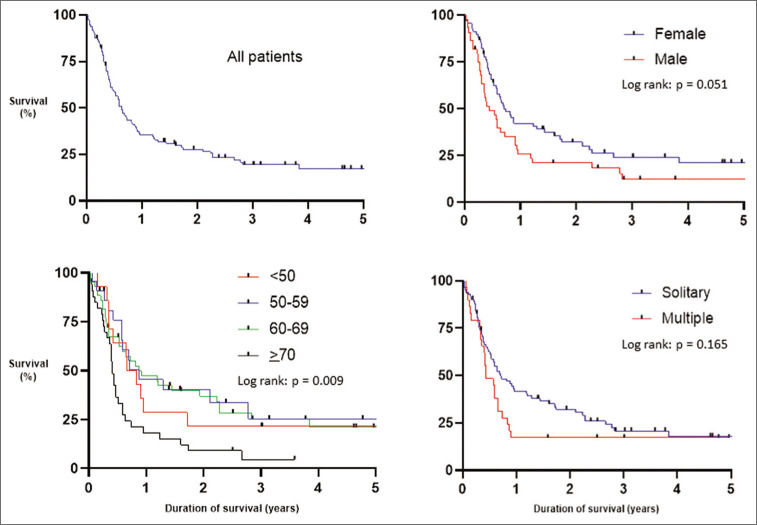
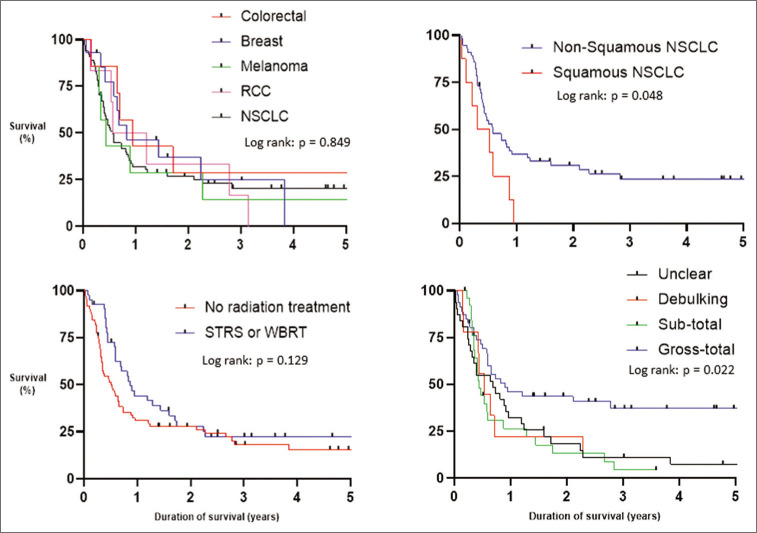
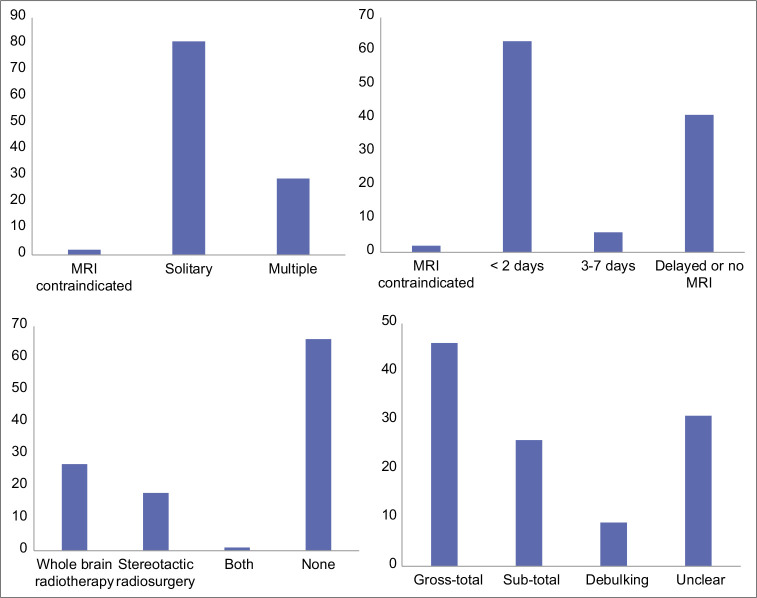
Methods: A retrospective case series including patients who underwent resection of cranial metastases from March 2014 to April 2021 at a single center. This identified 112 patients who underwent 124 resections. The median age was 65 years old (24-84) and the most frequent primary cancers were nonsmall cell lung cancer (56%), breast adenocarcinoma (13%), melanoma (6%), and colorectal adenocarcinoma (6%). Postoperative MRI with contrast was performed within 48 hours in 56% of patients and radiation treatment was administered in 41%. GraphPad Prism 9.2.0 was used for the survival analysis.
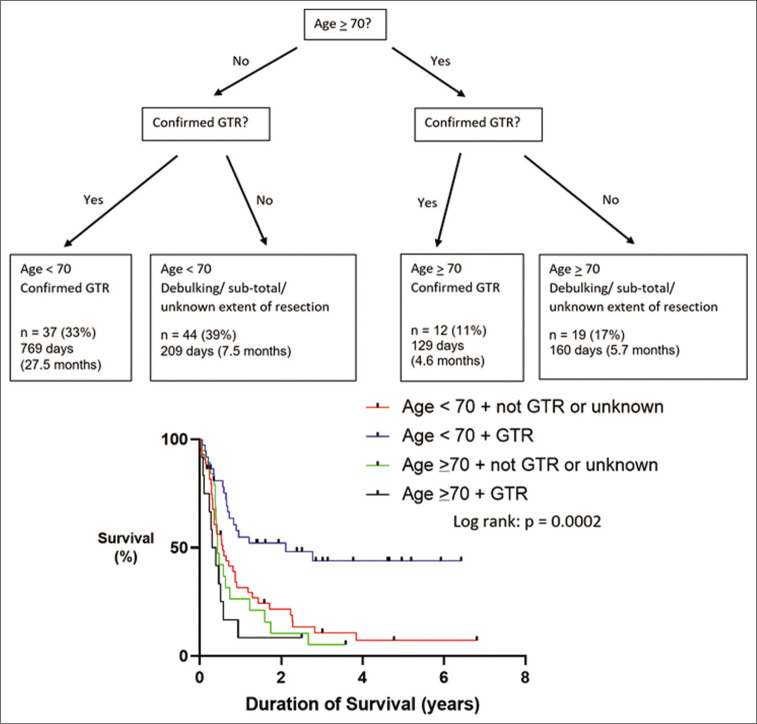
Results: At the time of data collection, 23% were still alive with a median follow-up of 1070 days (68-2484). The 30- and 90-day, and 1- and 5-year overall survival rates were 93%, 83%, 35%, and 17%, respectively. The most common causes of death within 90 days were as follows: unknown (32%), systemic or intracranial disease progression (26%), and pneumonia (21%). Age and extent of neurosurgical resection were associated with overall survival (P < 0.05). Patients aged >70 had a median survival of 5.4 months compared with 9.7, 11.4, and 11.4 for patients <50, 50-59, and 60-69, respectively. Gross-total resection achieved an overall survival of 11.8 months whereas sub-total, debulking, and unclear extent of resection led to a median survival of 5.7, 7.0, and 9.0 months, respectively.
Conclusion: Age and extent of resection are potential predictors of long-term survival.
Keywords: Brain metastasis; Breast cancer; Nonsmall cell lung cancer; Stereotactic radiosurgery; Whole-brain radiotherapy.
Copyright: © 2022 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Survival after surgery and stereotactic radiosurgery for patients with multiple intracranial metastases: results of a single-center retrospective study.J Neurosurg. 2014 Oct;121(4):839-45. doi: 10.3171/2014.4.JNS13789. Epub 2014 May 23. J Neurosurg. 2014. PMID: 24857242
-
Stereotactic radiosurgery to the resection bed for intracranial metastases and risk of leptomeningeal carcinomatosis.J Neurosurg. 2014 Dec;121 Suppl:75-83. doi: 10.3171/2014.6.GKS14708. J Neurosurg. 2014. PMID: 25434940
-
Postoperative stereotactic radiosurgery to the resection cavity for large brain metastases: clinical outcomes, predictors of intracranial failure, and implications for optimal patient selection.Neurosurgery. 2015 Feb;76(2):150-6; discussion 156-7; quiz 157. doi: 10.1227/NEU.0000000000000584. Neurosurgery. 2015. PMID: 25549189
-
Properly selected patients with multiple brain metastases may benefit from aggressive treatment of their intracranial disease.J Neurooncol. 2003 Jan;61(1):73-80. doi: 10.1023/a:1021262218151. J Neurooncol. 2003. PMID: 12587798 Review.
-
Stereotactic radiosurgery versus stereotactic radiotherapy in the management of intracranial meningiomas: a systematic review and meta-analysis.Neurosurg Focus. 2019 Jun 1;46(6):E2. doi: 10.3171/2019.3.FOCUS1970. Neurosurg Focus. 2019. PMID: 31153149
Cited by
-
Role of microsurgical tumor burden reduction in patients with breast cancer brain metastases considering molecular subtypes: a two-center volumetric survival analysis.J Neurooncol. 2024 Sep;169(2):379-390. doi: 10.1007/s11060-024-04728-w. Epub 2024 Jun 3. J Neurooncol. 2024. PMID: 38829577 Free PMC article.
References
-
- Al-Shamy G, Sawaya R. Management of brain metastases: The indispensable role of surgery. J Neurooncol. 2009;92:275–82. - PubMed
-
- Banfill KE, Bownes PJ, St Clair SE, Loughrey C, Hatfield P. Stereotactic radiosurgery for the treatment of brain metastases: Impact of cerebral disease burden on survival. Br J Neurosurg. 2012;26:674–8. - PubMed
-
- Brown PD, Ballman KV, Cerhan JH, Anderson SK, Carrero XW, Whitton AC, et al. Postoperative stereotactic radiosurgery compared with whole brain radiotherapy for resected metastatic brain disease (NCCTG N107C/CEC·3): A multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2017;18:1049–60. - PMC - PubMed
-
- D’Andrea G, Palombi L, Minniti G, Pesce A, Marchetti P. Brain metastases: Surgical treatment and overall survival. World Neurosurg. 2017;97:169–77. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous