

Uterine myxoid leiomyosarcoma - a rare malignant tumor: the role of complex morphopathological assay. Review and case presentation
- PMID: 35673808
- PMCID: PMC9289713
- DOI: 10.47162/RJME.62.4.01
Uterine myxoid leiomyosarcoma - a rare malignant tumor: the role of complex morphopathological assay. Review and case presentation
Abstract
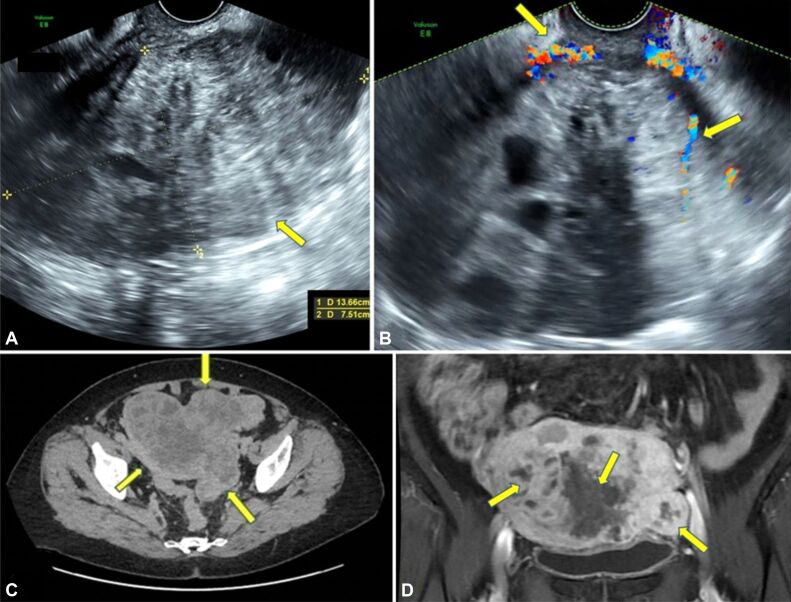
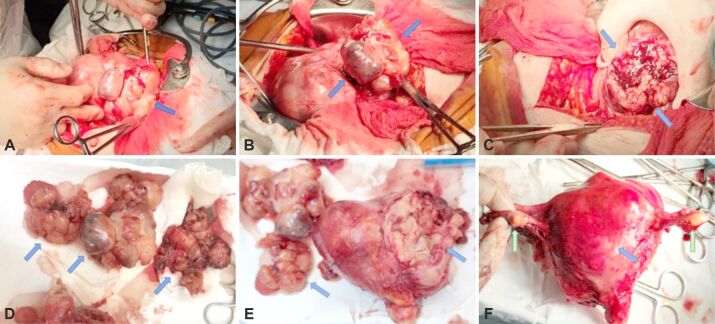
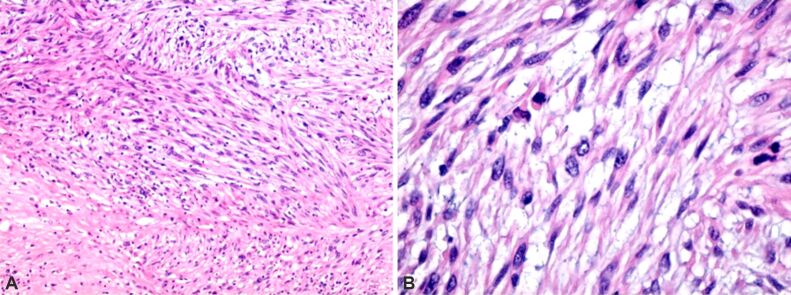
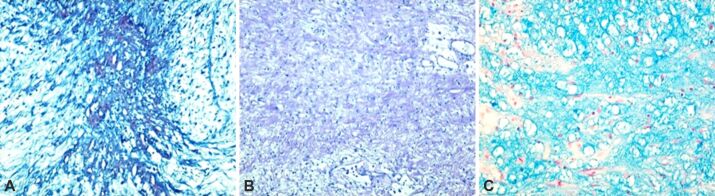
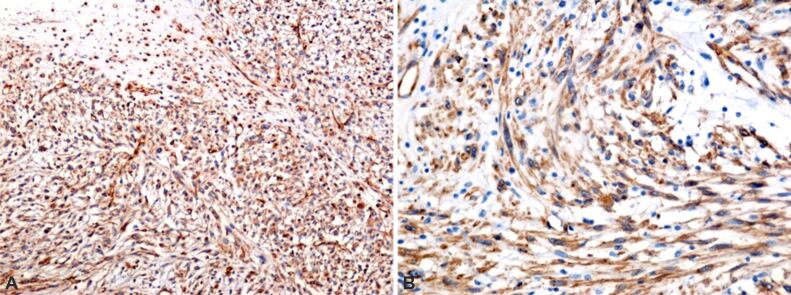
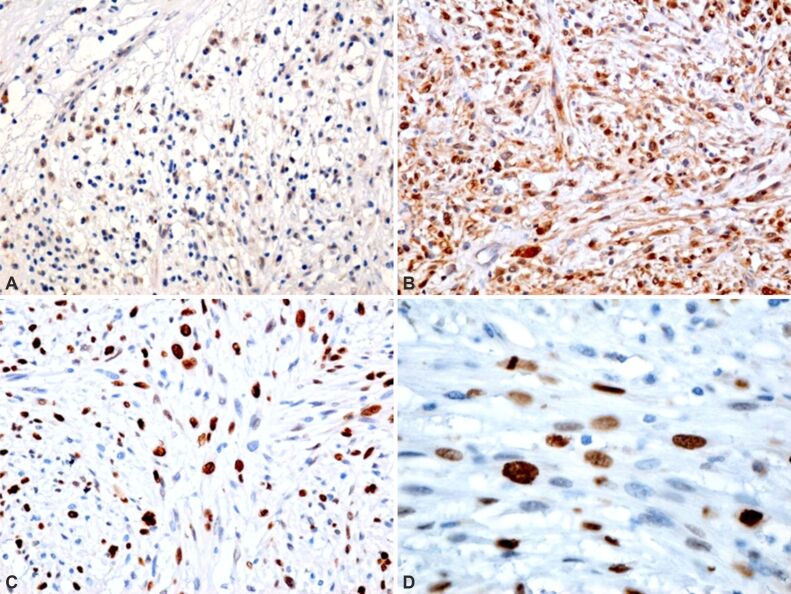
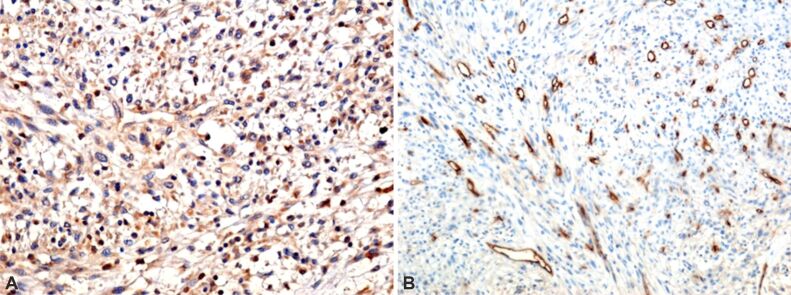
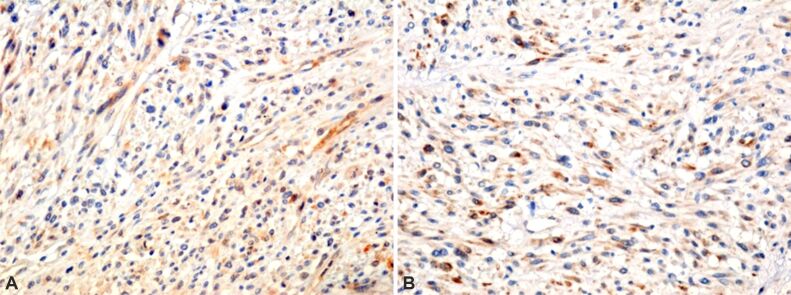
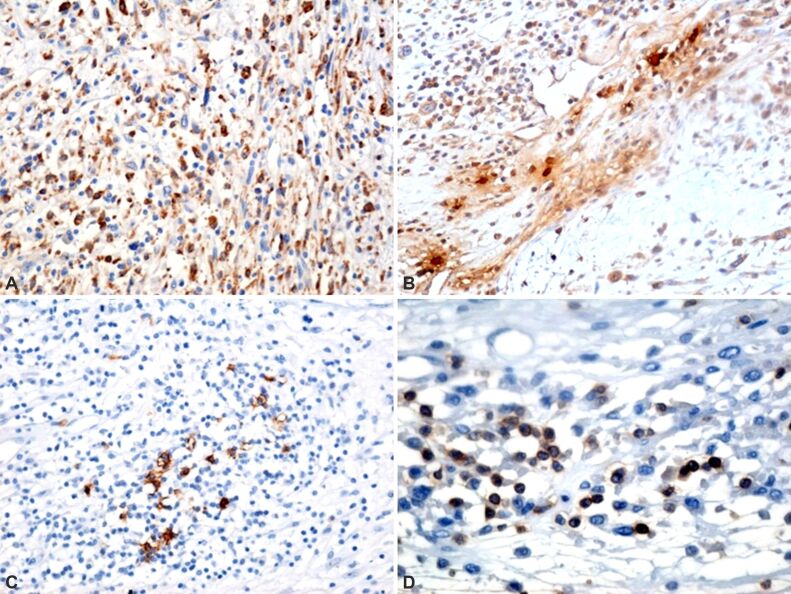
Malignant mixed mesodermal sarcomas (myxoid leiomyosarcomas - MLMS) are a rare form of uterine cancer developed from the smooth muscles of the uterus. It usually affects women in the postmenopausal period and has an aggressive character with an unfavorable evolution and prognosis. This paper presents a case where MLMS was postoperatively confirmed with the aid of the histopathological (HP) examination coupled with specific immunolabeling techniques. In addition, we reviewed modern literature to compare our results. Clinically, patients may present with a pelvic tumor, vaginal bleeding, or abdominal pressure. Imagistic investigations, such as pelvic ultrasonography (US), computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET)-CT may support the diagnosis. Nevertheless, solely the HP examination establishes it. Macroscopically, MLMS is soft and gelatinous, unlike the conventional rigid and spiral leiomyoma appearance. Furthermore, the infiltrative, irregular tumor margin is characteristic of MLMS. From a microscopic point of view, the following are present: tumor cell necrosis, nuclear pleomorphism, and variable mitotic activity. With classical Hematoxylin-Eosin (HE) staining, myometrium presents a leiomyomatous structure and multiple nodular formations with the aspect of malignant tumor proliferation, most likely mesenchymal. We used multiple special immunolabeling techniques. Thus, we observed the intense reactivity of the cells to the anti-vimentin antibody, which immunolabeled type III intermediate filament (IF) protein expressed in mesenchymal cells, thus demonstrating tumor mesenchymal affiliation. Smooth cell positivity for alpha-smooth muscle actin (α-SMA) demonstrates that the tumor is present in its whole myometrial structure. Tumor cells also underwent mutations involving the p53 tumor suppressor gene demonstrated by the number of tumoral cells in division immunolabeled with anti-Ki67 proliferation antibody. Tumor development was demonstrated by protein activation of cyclin-dependent kinase (CDK) and the presence of c-Kit-bound hematopoietic stem cells, immunolabeled with the anti-cluster of differentiation 117 (anti-CD117) antibodies. The anti-desmin antibody demonstrates, along with α-SMA, the involvement of myocytes in the tumoral process. The following microscopic characteristics laid the foundation for the diagnosis of MLMS: irregular myometrial invasion, rare mitosis on high-power fields (HPFs), cell pleomorphism, predominant myxoid component that gave a hypocellular appearance, the matrix rich in proteoglycans and glycosaminoglycans, especially hyaluronic acid.
Conflict of interest statement
The authors declare that they have no conflict of interests.
Figures
Similar articles
-
Myxoid Leiomyosarcoma of the Uterus: A Clinicopathologic Analysis of 30 Cases and Review of the Literature With Reappraisal of Its Distinction From Other Uterine Myxoid Mesenchymal Neoplasms.Am J Surg Pathol. 2016 Mar;40(3):285-301. doi: 10.1097/PAS.0000000000000593. Am J Surg Pathol. 2016. PMID: 26866354 Review.
-
P16, Ki67, P53, and WT1 Expression in Uterine Smooth Muscle Tumors: An Adjunct in Confirming the Diagnosis of Malignancy in Ambiguous Cases.Int J Gynecol Pathol. 2021 May 1;40(3):257-262. doi: 10.1097/PGP.0000000000000688. Int J Gynecol Pathol. 2021. PMID: 32897968
-
[Mesenchymal uterine tumors. Leiomyomas].Pathologe. 2009 Jul;30(4):274-83. doi: 10.1007/s00292-009-1160-1. Pathologe. 2009. PMID: 19495761 German.
-
Myxoid leiomyosarcoma of the uterus.Histopathology. 2011 Dec;59(6):1144-55. doi: 10.1111/j.1365-2559.2011.04053.x. Histopathology. 2011. PMID: 22175894
-
Pleomorphic Undifferentiated Uterine Sarcoma in a Young Patient Presenting With Elevated Beta-hCG and Rare Variants of Benign Leiomyoma: A Case Report and Review of the Literature.Int J Gynecol Pathol. 2020 Jul;39(4):362-366. doi: 10.1097/PGP.0000000000000606. Int J Gynecol Pathol. 2020. PMID: 31033798 Review.
Cited by
-
Myxoid leiomyosarcoma of the uterus in a woman of childbearing age: A case report.Oncol Lett. 2025 Apr 2;29(6):264. doi: 10.3892/ol.2025.15010. eCollection 2025 Jun. Oncol Lett. 2025. PMID: 40230424 Free PMC article.
References
-
- Papadopoulos AJ, Kenney A. Solid malignant uterine tumours. Curr Obstet Gynaecol. 2001;11(5):296–301. https://www.sciencedirect.com/science/article/abs/pii/S0957584701901994?...
-
- King ME, Dickersin GR, Scully RE. Myxoid leiomyosarcoma of the uterus. A report of six cases. Am J Surg Pathol. 1982;6(7):589–598. - PubMed
-
- Burch DM, Tavassoli FA. Myxoid leiomyosarcoma of the uterus. Histopathology. 2011;59(6):1144–1155. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
