

CXCR4-targeted theranostics in oncology
- PMID: 35674738
- PMCID: PMC9525349
- DOI: 10.1007/s00259-022-05849-y
CXCR4-targeted theranostics in oncology
Abstract
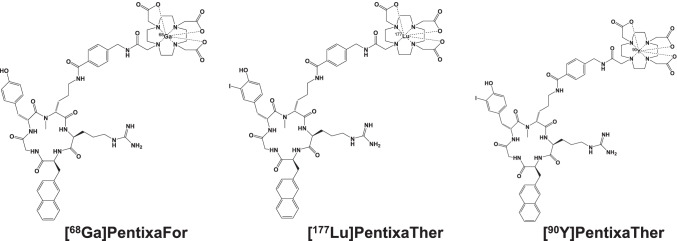
A growing body of literature reports on the upregulation of C-X-C motif chemokine receptor 4 (CXCR4) in a variety of cancer entities, rendering this receptor as suitable target for molecular imaging and endoradiotherapy in a theranostic setting. For instance, the CXCR4-targeting positron emission tomography (PET) agent [68 Ga]PentixaFor has been proven useful for a comprehensive assessment of the current status quo of solid tumors, including adrenocortical carcinoma or small-cell lung cancer. In addition, [68 Ga]PentixaFor has also provided an excellent readout for hematological malignancies, such as multiple myeloma, marginal zone lymphoma, or mantle cell lymphoma. PET-based quantification of the CXCR4 capacities in vivo allows for selecting candidates that would be suitable for treatment using the theranostic equivalent [177Lu]/[90Y]PentixaTher. This CXCR4-directed theranostic concept has been used as a conditioning regimen prior to hematopoietic stem cell transplantation and to achieve sufficient anti-lymphoma/-tumor activity in particular for malignant tissues that are highly sensitive to radiation, such as the hematological system. Increasing the safety margin, pretherapeutic dosimetry is routinely performed to determine the optimal activity to enhance therapeutic efficacy and to reduce off-target adverse events. The present review will provide an overview of current applications for CXCR4-directed molecular imaging and will introduce the CXCR4-targeted theranostic concept for advanced hematological malignancies.
Keywords: Adrenocortical carcinoma; C-X-C motif chemokine receptor 4; CXCR4; Endoradiotherapy; Multiple myeloma; Theranostics; [177Lu]PentixaTher; [68Ga]PentixaFor; [90Y]PentixaTher.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
