

Analysis of a Trend Reversal in US Lumpectomy Rates From 2005 Through 2017 Using 3 Nationwide Data Sets
- PMID: 35675047
- PMCID: PMC9178497
- DOI: 10.1001/jamasurg.2022.2065
Analysis of a Trend Reversal in US Lumpectomy Rates From 2005 Through 2017 Using 3 Nationwide Data Sets
Abstract
Importance: Rates of lumpectomy for breast cancer management in the United States previously declined in favor of more aggressive surgical options, such as mastectomy and contralateral prophylactic mastectomy (CPM).
Objective: To evaluate longitudinal trends in the rates of lumpectomy and mastectomy, including unilateral mastectomy vs CPM rates, and to determine characteristics associated with current surgical practice using 3 national data sets.
Design and setting: Data from the National Surgical Quality Improvement Program (NSQIP), Surveillance, Epidemiology, and End Results (SEER) program, and National Cancer Database (NCDB) were examined to evaluate trends in lumpectomy and mastectomy rates from 2005 through 2017. Mastectomy rates were also evaluated with a focus on CPM. Longitudinal trends were analyzed using the Cochran-Armitage test for trend. Multivariate logistic regression models were performed on the NCDB data set to identify predictors of lumpectomy and CPM.
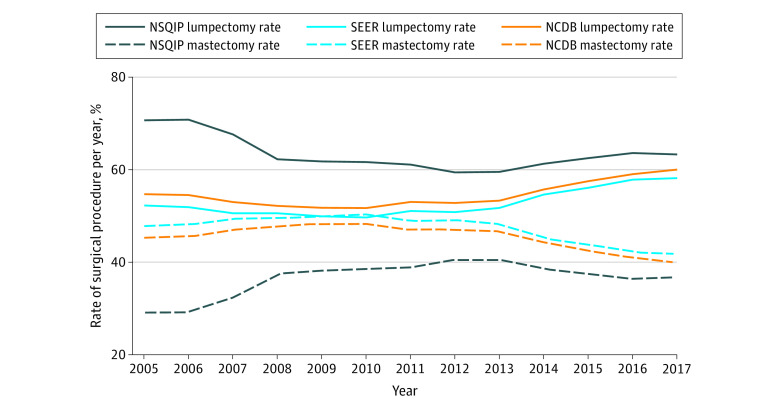
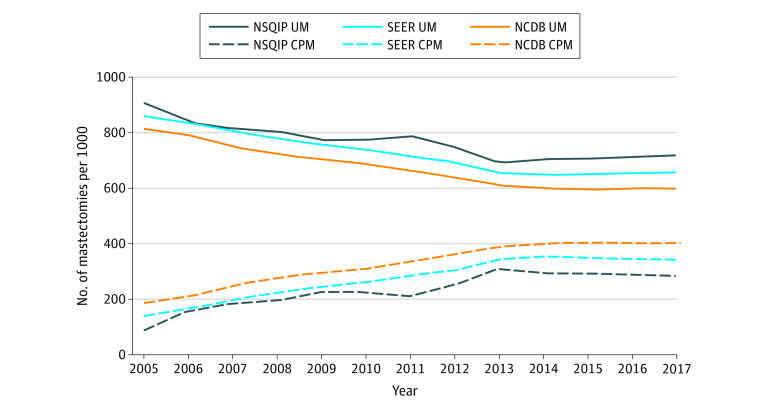
Results: A study sample of 3 467 645 female surgical breast cancer patients was analyzed. Lumpectomy rates reached a nadir between 2010 and 2013, with a significant increase thereafter. Conversely, in comparison with lumpectomy rates, overall mastectomy rates declined significantly starting in 2013. Cochran-Armitage trend tests demonstrated an annual decrease in lumpectomy rates of 1.31% (95% CI, 1.30%-1.32%), 0.07% (95% CI, 0.01%-0.12%), and 0.15% (95% CI, 0.15%-0.16%) for NSQIP, SEER, and NCDB, respectively, from 2005 to 2013 (P < .001, P = .01, and P < .001, respectively). From 2013 to 2017, the annual increase in lumpectomy rates was 0.96% (95% CI, 0.95%-0.98%), 1.60% (95% CI, 1.59%-1.62%), and 1.66% (95% CI, 1.65%-1.67%) for NSQIP, SEER, and NCDB, respectively (all P < .001). Comparisons of specific mastectomy types showed that unilateral mastectomy and CPM rates stabilized after 2013, with unilateral mastectomy rates remaining higher than CPM rates throughout the entire time period.
Conclusions: This observational longitudinal analysis indicated a trend reversal with an increase in lumpectomy rates since 2013 and an associated decline in mastectomies. The steady increase in CPM rates from 2005 to 2013 has since stabilized. The reasons for the recent reversal in trends are likely multifactorial. Further qualitative and quantitative research is required to understand the factors driving these recent practice changes and their associations with patient-reported outcomes.
Conflict of interest statement
Figures
Comment in
-
Surgical Decision-making in Early-Stage Breast Cancer-Trends and Opportunities.JAMA Surg. 2022 Aug 1;157(8):711-712. doi: 10.1001/jamasurg.2022.2072. JAMA Surg. 2022. PMID: 35675045 No abstract available.
References
-
- Fisher B, Montague E, Redmond C, et al. Comparison of radical mastectomy with alternative treatments for primary breast cancer: a first report of results from a prospective randomized clinical trial. Cancer. 1977;39(6)(suppl):2827-2839. doi: 10.1002/1097-0142(197706)39:6<2827::AID-CNCR2820390671>3.0.CO;2-I - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
