

Emergency vs Delayed Coronary Angiogram in Survivors of Out-of-Hospital Cardiac Arrest: Results of the Randomized, Multicentric EMERGE Trial
- PMID: 35675081
- PMCID: PMC9178496
- DOI: 10.1001/jamacardio.2022.1416
Emergency vs Delayed Coronary Angiogram in Survivors of Out-of-Hospital Cardiac Arrest: Results of the Randomized, Multicentric EMERGE Trial
Abstract
Importance: Although an emergency coronary angiogram (CAG) is recommended for patients who experience an out-of-hospital cardiac arrest (OHCA) with ST-segment elevation on the postresuscitation electrocardiogram (ECG), this strategy is still debated in patients without ST-segment elevation.
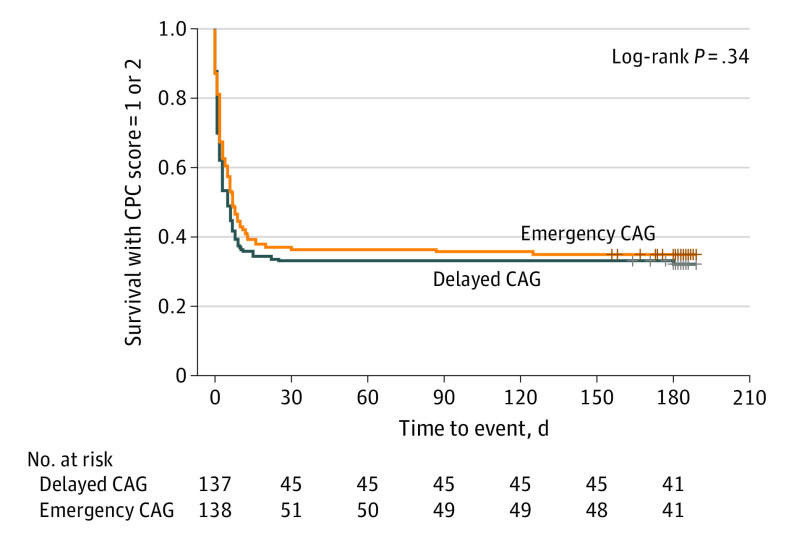
Objective: To assess the 180-day survival rate with Cerebral Performance Category (CPC) 1 or 2 of patients who experience an OHCA without ST-segment elevation on ECG and undergo emergency CAG vs delayed CAG.
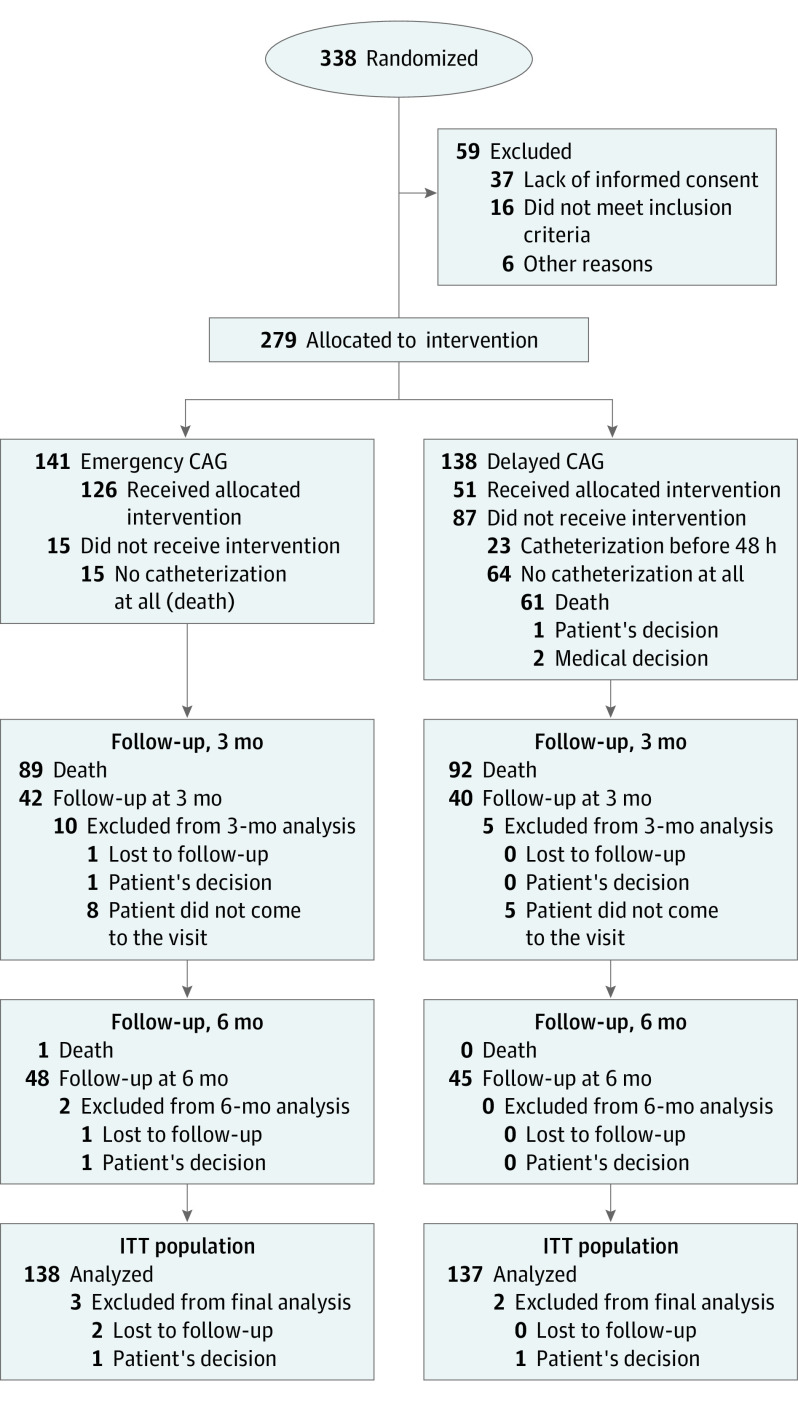
Design, setting, and participants: The Emergency vs Delayed Coronary Angiogram in Survivors of Out-of-Hospital Cardiac Arrest (EMERGE) trial randomly assigned survivors of an OHCA without ST-segment elevation on ECG to either emergency or delayed (48 to 96 hours) CAG in 22 French centers. The trial took place from January 19, 2017, to November 23, 2020. Data were analyzed from November 24, 2020, to July 30, 2021.
Main outcomes and measures: The primary outcome was the 180-day survival rate with CPC of 2 or less. The secondary end points were occurrence of shock, ventricular tachycardia, and/or fibrillation within 48 hours, change in left ventricular ejection fraction between baseline and 180 days, CPC scale at intensive care unit discharge and day 90, survival rate, and hospital length of stay.
Results: A total of 279 patients (mean [SD] age, 64.7 [14.6] years; 195 men [69.9%]) were enrolled, with 141 (50.5%) in the emergency CAG group and 138 (49.5%) in the delayed CAG group. The study was underpowered. The mean (SD) time delay between randomization and CAG was 0.6 (3.7) hours in the emergency CAG group and 55.1 (37.2) hours in the delayed CAG group. The 180-day survival rates among patients with a CPC of 2 or less were 34.1% (47 of 141) in the emergency CAG group and 30.7% (42 of 138) in the delayed CAG group (hazard ratio [HR], 0.87; 95% CI, 0.65-1.15; P = .32). There was no difference in the overall survival rate at 180 days (emergency CAG, 36.2% [51 of 141] vs delayed CAG, 33.3% [46 of 138]; HR, 0.86; 95% CI, 0.64-1.15; P = .31) and in secondary outcomes between the 2 groups.
Conclusions and relevance: In this randomized clinical trial, for patients who experience an OHCA without ST-segment elevation on ECG, a strategy of emergency CAG was not better than a strategy of delayed CAG with respect to 180-day survival rate and minimal neurologic sequelae.
Trial registration: ClinicalTrials.gov Identifier: NCT02876458.
Conflict of interest statement
Figures

References
-
- Lloyd-Jones D, Adams RJ, Brown TM, et al. ; WRITING GROUP MEMBERS; American Heart Association Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2010 update: a report from the American Heart Association. Circulation. 2010;121(7):e46-e215. doi: 10.1161/CIRCULATIONAHA.109.192667 - DOI - PubMed
-
- Writing Group Members; Mozaffarian D, Benjamin EJ, Go AS, et al. ; American Heart Association Statistics Committee; Stroke Statistics Subcommittee . Heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38-e360. doi: 10.1161/CIR.0000000000000350 - DOI - PubMed
-
- Nichol G, Baker D. The epidemiology of sudden death. In: Paradis NA, Halperin HR, Kern KB, Wenzel V, Chamberlain DA, eds. Cardiac Arrest—The Science and Practice of Resuscitation Medicine. Cambridge University Press; 2007:26-48.
