

External Support for Saphenous Vein Grafts in Coronary Artery Bypass Surgery: A Randomized Clinical Trial
- PMID: 35675092
- PMCID: PMC9178499
- DOI: 10.1001/jamacardio.2022.1437
External Support for Saphenous Vein Grafts in Coronary Artery Bypass Surgery: A Randomized Clinical Trial
Abstract
Importance: Intimal hyperplasia and subsequent saphenous vein graft failure may have significant adverse clinical effects in patients undergoing coronary artery bypass surgery. External support of saphenous vein grafts has the potential to prevent vein graft dilation and hence slow the rate of intimal hyperplasia and increase long-term vein patency.
Objective: To determine efficacy, as measured by intimal hyperplasia, and safety of an external saphenous vein graft support device in patients undergoing a coronary bypass graft procedure.
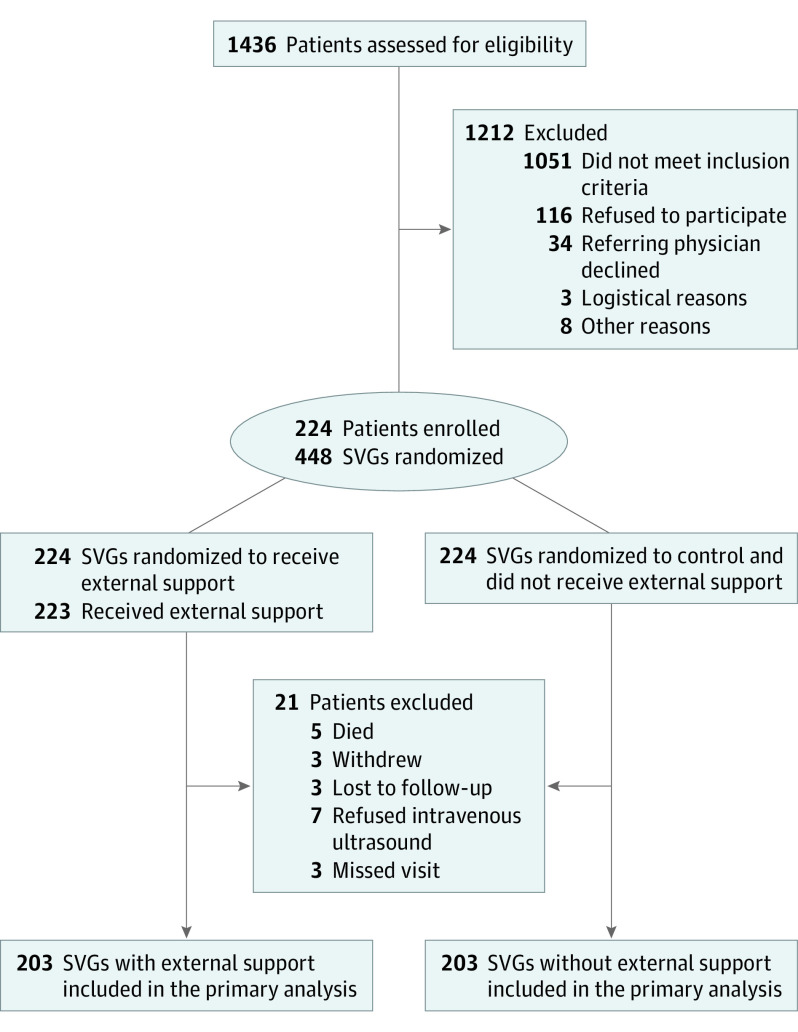
Design, setting, and participants: This within-patient randomized, open-label, multicenter study was conducted at 17 Cardiothoracic Surgical Trials Network centers in North America. Between January 2018 and February 2019, 224 patients with multivessel coronary artery disease undergoing isolated bypass surgery were enrolled. For each patient, 1 of 2 vein grafts was randomized to receive external support or no support.
Interventions: External vein graft support or no support.
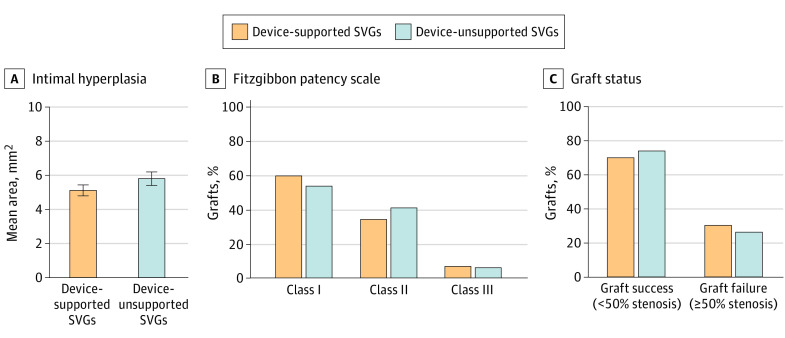
Main outcomes and measures: The primary efficacy end point was intimal hyperplasia area assessed by intravascular ultrasound at 12 months postrandomization for each study graft. Secondary confirmatory end points were lumen diameter uniformity assessed by angiography and graft failure (≥50% stenosis) by quantitative coronary angiography. Major cardiac and cerebrovascular events were collected through month 12.
Results: Among 224 patients (mean [SD] age, 65.8 [8.3] years; 178 [79.5%] male), 203 (90.6%) were eligible for intravascular ultrasound, of which 85 (41.9%) had at least 1 study graft occluded or severely diseased at 12 months (55 supported, 56 unsupported). After imputation of data missing because of graft occlusion or severe disease, the estimated mean (SE) intimal hyperplasia area was 5.11 (0.16) mm2 in supported grafts and 5.79 (0.20) mm2 in unsupported grafts (P = .07). In a sensitivity analysis of 113 patients with both grafts imaged, the mean intimal hyperplasia area was 4.58 (0.18) mm2 and 5.12 (0.23) mm2 in supported and unsupported grafts, respectively (P = .04). By 12 months, 5 patients (2.2%) died and 16 patients (7.1%) experienced a major cardiac or cerebrovascular event.
Conclusions and relevance: The 12-month difference in intimal hyperplasia area between supported and unsupported grafts did not achieve statistical significance. Cumulative mortality and major cardiac or cerebrovascular events rates were similar to those in other randomized coronary artery bypass trials. Further investigation to assess the effect of external graft support devices on long-term graft patency and clinical outcomes is warranted.
Trial registration: ClinicalTrials.gov Identifier: NCT03209609.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
