

Long-term Outcomes of Local and Metastatic Small Cell Carcinoma of the Urinary Bladder and Genomic Analysis of Patients Treated With Neoadjuvant Chemotherapy
- PMID: 35676169
- PMCID: PMC9809986
- DOI: 10.1016/j.clgc.2022.05.005
Long-term Outcomes of Local and Metastatic Small Cell Carcinoma of the Urinary Bladder and Genomic Analysis of Patients Treated With Neoadjuvant Chemotherapy
Abstract
Introduction: Small cell carcinoma of the bladder (SCCB) is a rare variant of bladder cancer with poor outcomes. We evaluated long-term outcomes of nonmetastatic (M0) and metastatic (M1) SCCB and correlated pathologic response with genomic alterations of patients treated with neoadjuvant chemotherapy (NAC).
Patients and methods: Clinical history and pathology samples from SCCB patients diagnosed at our institution were reviewed.
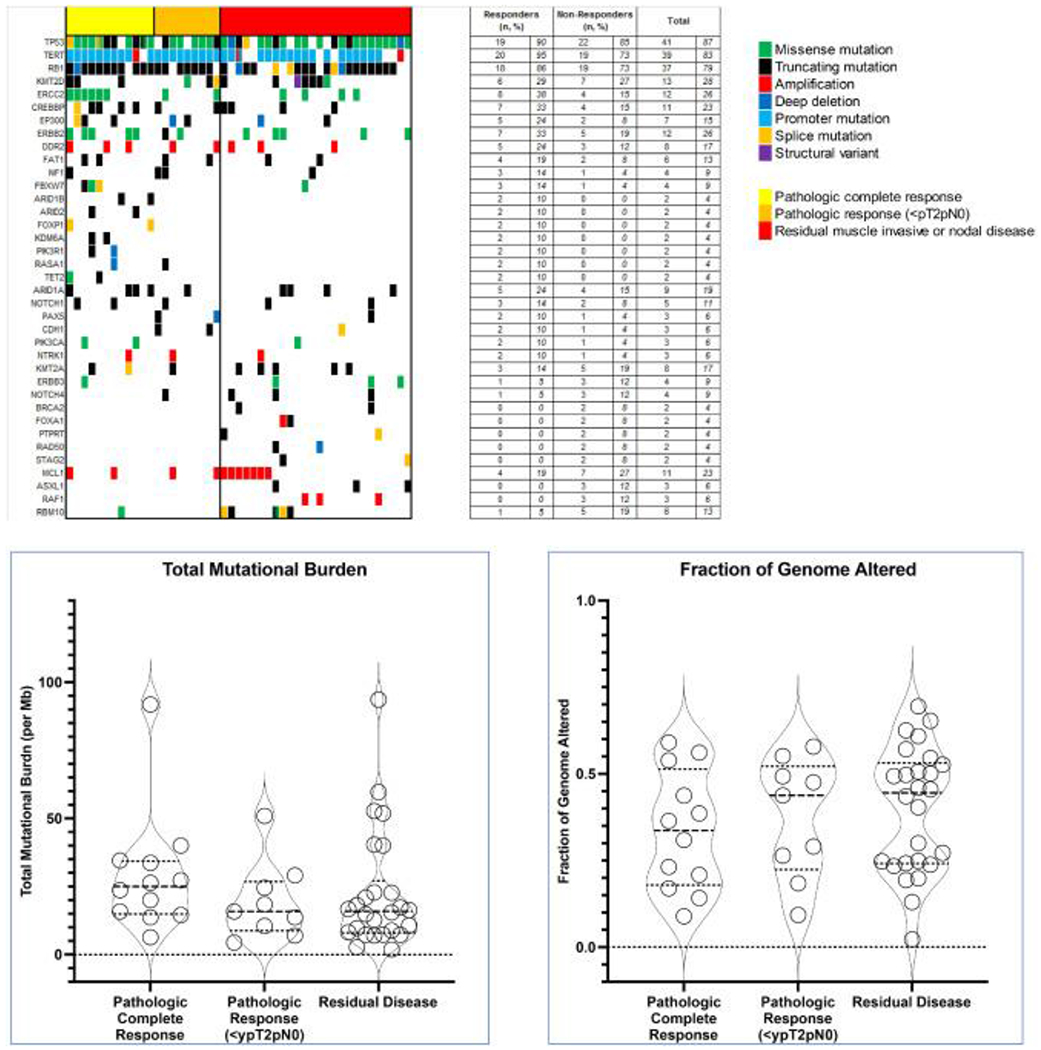
Results: One hundred and ninety-nine SCCB patients were identified. (M0: 147 [74%]; M1: 52 [26%]). Among M0 patients, 108 underwent radical cystectomy (RC) (NAC: 71; RC only: 23; adjuvant chemotherapy: 14); 14 received chemoradiotherapy; the rest received chemotherapy alone or no cancer-directed therapy. RC-only patients had a median follow-up of 9.1 years, and median disease-free survival (DFS) and overall survival (OS) were 1.1 and 1.2 years, respectively. NAC patients had pathologic response (<pT2pN0) and pathologic complete response (pT0pN0) rates of 48% and 38%, respectively, with median follow-up of 7.2 years, and median DFS and OS of 5.6 and 14.5 years, respectively. NAC responders (<ypT2N0) had superior median DFS (14.5 vs. 0.6 years, hazard ratio [HR] 0.24, P< .001) and OS (14.5 vs. 2.5 years, HR 0.31, P = .002). DFS rates for responders and nonresponders were 76% and 27% at 5 years, and 71% and 23% at 10 years, respectively. Local and central nervous system recurrences were infrequent. Median progression-free survival (PFS) and OS for M1 disease were 6.9 and 10.3 months, respectively. Genomic profiling was performed on 47 NAC patients. Loss of ERCC2 function was significantly enriched among those with pathologic complete response to NAC (mutations present in 50% of pathologic complete responders vs. 15% nonresponders, P = .045).
Conclusion: M0 SCCB is chemo-sensitive and patients have excellent long-term survival following response to NAC. Patients with M1 disease have poor survival despite systemic therapy. Loss-of-function mutations of ERCC2 were associated with pathologic complete response to NAC.
Keywords: Bladder cancer; Neuroendocrine carcinoma; Radical cystectomy; Small cell bladder cancer; Urothelial carcinoma.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure M.Y. Teo reports consulting/advisory role for Janssen Oncology and institutional research funding from Bristol-Myers Squibb, Clovis Oncology, and Pharmacyclics. B.J. Guercio reports honoraria from Medscape and institutional research funding from Bristol-Myers Squibb, Genentech, Eli Lilly, Pfizer, and Sanofi. E. Pietzak reports receiving honoraria from UpToDate, has served on the Scientific Advisory Board for Janssen Pharmaceuticals, Merck & Co Inc., QED Therapeutics, Chugai Pharmaceuticals, and Steba Biotech, and receives research funding from Janssen Pharmaceuticals. B.H. Bochner reports consulting/advisory role for Genentech/Roche and Olympus; and honoraria from Genentech/Roche. A.C. Goh has served as a consultant for Medtronic. B. Weigelt reports ad hoc membership of the scientific advisory board of Repare Therapeutics, outside the submitted study. J. Sarungbam reports work as a consultant for Janssen Research & Development, LLC. S.A. Funt receives research funding from AstraZeneca and Genetech/Roche, has consulted for/received honoraria from Merck and has stock/equity ownership in Allogene Therapeutics, Urogen, Kronos Bio, Neogene Therapeutics, IconOVir, Vida Ventures, Doximity, and Ginkgo Bioworks. D.F. Bajorin reports personal fees from Bristol Myers Squibb and Merck; consulting/advisory role for Merck, Dragonfly Therapeutics, Fidia Farmaceutici S.p.A., and Bristol Myers Squibb Foundation; Travel/accommodations/expenses from Merck; and institutional research funding from Novartis, Merck, Bristol-Myers Squibb, AstraZeneca, Astellas Pharma, and Seattle Genetics/Astellas. D.B. Solit reports personal fees from BridgeBio, Loxo/Lilly Oncology, Scorpion Therapeutics, Vividion Therapeutics, Pfizer, and FORE Therapeutics outside the submitted work. G. Iyer reports institutional research funding from Novartis, Bayer, Debiopharm, Seagen, Inc, Mirati Therapeutics, and Janssen; has served as a consultant or advisory role for Bayer, Janssen, Mirtai Therapeutics, Basilea, Flare Therapeutics, and Loxo/Lilly; has served as a speaker for Gilead Sciences and the Lynx Group; and has received personal fees from Personal fees from LOXO Oncology, Flare Therapeutics, Gilead, The Lynx Group, and DAVA Oncology. J.E. Rosenberg reports honoraria from Clinical Care Options, Medscape, Peerview, Physicans' Education Resource, Research To Practice, UpToDate, and EMD-Serono; consulting or advisory role for Astellas Pharma, AstraZeneca, Bayer, BioClin Therapeutics, Boehringer Ingelheim, Bristol-Myers Squibb, GlaxoSmithKline, Gilead/Immunomedics, Infinity, Janssen Oncology, Lilly, Merck, Mirati Therapeutics, Pfizer, EMD Serono, Pharmacyclics, Roche/Genentech, Seagen, and QED Therapeutics; institutional research funding from Astellas Pharma, AstraZeneca, Bayer, Genentech/Roche, Seagen, and QED Therapeutics; and an institutional patent regarding prediction of platinum sensitivity. H. Al-Ahmadie reports consulting/advisory roles for Bristol-Myers Squibb, EMD Serono, AstraZeneca/MedImmune, Janssen Biotech, and PAIGE.AI. The remaining authors have no relevant conflicts of interest/ disclosures to report.
Figures


References
-
- Naidoo J, Teo MY, Deady S, Comber H, Calvert P. Should patients with extrapulmonary small-cell carcinoma receive prophylactic cranial irradiation? J Thorac Oncol. 2013;8:1215–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
