

Phase I 270° single-incision percutaneous spinal endoscopy for decompression treatment of thoracic spinal stenosis
- PMID: 35676323
- PMCID: PMC9177758
- DOI: 10.1038/s41598-022-13666-4
Phase I 270° single-incision percutaneous spinal endoscopy for decompression treatment of thoracic spinal stenosis
Abstract
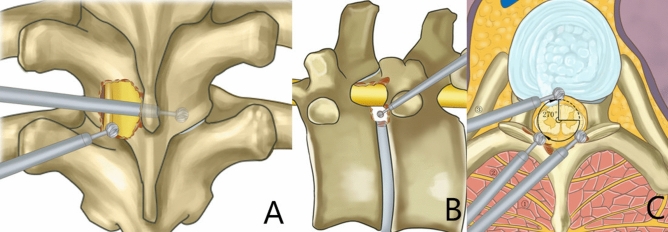
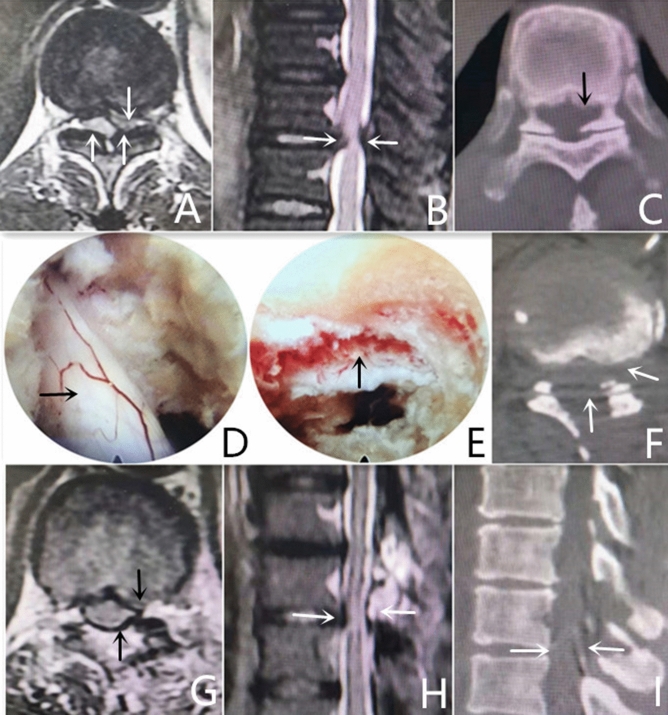
This study aimed to explore the feasibility of Phase I percutaneous spinal endoscopy with a 270° single incision in the ventral and dorsal dura mater for decompression treatment of thoracic spinal stenosis (TSS). Phase I percutaneous spinal endoscopy with a two-path (posterior and posterolateral approaches) single incision with a 270° decompression was performed in four cases of TSS with compression in the ventral and dorsal dura mater. The affected intervertebral space was located during the surgery, and the ossified ligamentum flavum in the ventral and dorsal dura mater was removed via laminectomy, which formed a decompression space in the thoracic cord. Next, posterolateral transforaminal expansion and plasty were performed to remove the ventral intervertebral disk. The visual analogue scale (VAS) score, thoracic spinal cord function score of the Japanese Orthopaedic Association (JOA) (11-point method), and Oswestry Disability Index (ODI) scores were used to evaluate the clinical efficacy. No dura mater or thoracic nerve injury occurred during the surgery. The symptoms of weakness in the lower extremities improved after the surgery. The postoperative magnetic resonance imaging and computed tomography examinations showed compression removal and dura mater bulging. The postoperative VAS, JOA, and ODI scores improved compared with the preoperative scores. Two surgical trajectories, posterior and posterolateral approaches, were established by a single incision using thoracic spinal canal decompression with Phase I 270° single-incision percutaneous spinal endoscopy. The posterior approach was performed mainly by translaminar unilateral fenestration and bilateral decompression in the ventral and dorsal dura mater, whereas the posterolateral approach was performed by decompression in the ventral dura mater to the midline of the vertebrae. This surgical method could be applied as a safe and feasible minimally invasive treatment for TSS with compression on both the ventral and dorsal dura mater.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Posterior Percutaneous Endoscopic Technique Through Bilateral Translaminar Osseous Channels for Thoracic Spinal Stenosis Caused by Ossification of the Ligamentum Flavum Combined with Disk Herniation at the T10-11 Level: A Technical Note.World Neurosurg. 2020 Jan;133:135-141. doi: 10.1016/j.wneu.2019.08.215. Epub 2019 Sep 7. World Neurosurg. 2020. PMID: 31505277
-
Fully Endoscopic 360° Decompression Surgery for Thoracic Spinal Stenosis: Technical Note and Report of 8 Cases.Pain Physician. 2020 Nov;23(6):E659-E663. Pain Physician. 2020. PMID: 33185384
-
Bilateral decompression and intervertebral fusion via unilateral fenestration for complex lumbar spinal stenosis with a mobile microendoscopic technique.Medicine (Baltimore). 2018 Jan;97(4):e9715. doi: 10.1097/MD.0000000000009715. Medicine (Baltimore). 2018. PMID: 29369203 Free PMC article.
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
Meta-Analysis of Simultaneous versus Staged Decompression of Stenotic Regions in Patients with Tandem Spinal Stenosis.World Neurosurg. 2023 Feb;170:e441-e454. doi: 10.1016/j.wneu.2022.11.028. Epub 2022 Nov 14. World Neurosurg. 2023. PMID: 36396060
Cited by
-
Endoscopy-assisted anterior cervical discectomy and fusion with internal fixation vs conventional surgery in the treatment of cervical disc herniation.Wideochir Inne Tech Maloinwazyjne. 2024 Jul 31;19(3):399-406. doi: 10.20452/wiitm.2024.17888. eCollection 2024 Oct 16. Wideochir Inne Tech Maloinwazyjne. 2024. PMID: 40041109 Free PMC article.
-
Morphometric Evaluation of Thoracolumbar Spinal Canal and Cord by Magnetic Resonance Imaging in Normal Small-Breed Dogs.Animals (Basel). 2024 Mar 28;14(7):1030. doi: 10.3390/ani14071030. Animals (Basel). 2024. PMID: 38612269 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
