

Prostate cancer therapy personalization via multi-modal deep learning on randomized phase III clinical trials
- PMID: 35676445
- PMCID: PMC9177850
- DOI: 10.1038/s41746-022-00613-w
Prostate cancer therapy personalization via multi-modal deep learning on randomized phase III clinical trials
Erratum in
-
Author Correction: Prostate cancer therapy personalization via multi-modal deep learning on randomized phase III clinical trials.NPJ Digit Med. 2023 Feb 22;6(1):27. doi: 10.1038/s41746-023-00769-z. NPJ Digit Med. 2023. PMID: 36813827 Free PMC article. No abstract available.
Abstract
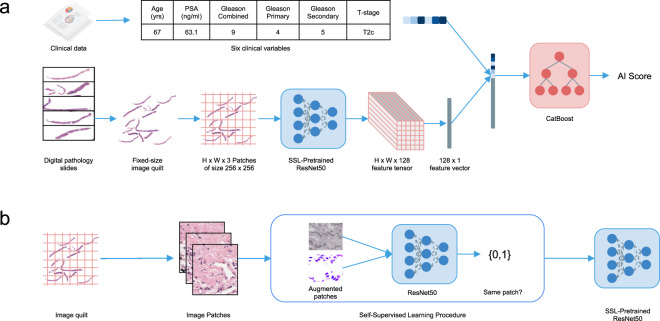
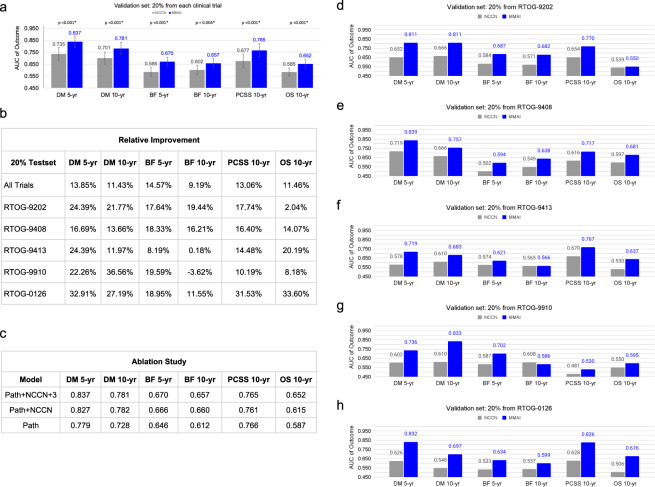
Prostate cancer is the most frequent cancer in men and a leading cause of cancer death. Determining a patient's optimal therapy is a challenge, where oncologists must select a therapy with the highest likelihood of success and the lowest likelihood of toxicity. International standards for prognostication rely on non-specific and semi-quantitative tools, commonly leading to over- and under-treatment. Tissue-based molecular biomarkers have attempted to address this, but most have limited validation in prospective randomized trials and expensive processing costs, posing substantial barriers to widespread adoption. There remains a significant need for accurate and scalable tools to support therapy personalization. Here we demonstrate prostate cancer therapy personalization by predicting long-term, clinically relevant outcomes using a multimodal deep learning architecture and train models using clinical data and digital histopathology from prostate biopsies. We train and validate models using five phase III randomized trials conducted across hundreds of clinical centers. Histopathological data was available for 5654 of 7764 randomized patients (71%) with a median follow-up of 11.4 years. Compared to the most common risk-stratification tool-risk groups developed by the National Cancer Center Network (NCCN)-our models have superior discriminatory performance across all endpoints, ranging from 9.2% to 14.6% relative improvement in a held-out validation set. This artificial intelligence-based tool improves prognostication over standard tools and allows oncologists to computationally predict the likeliest outcomes of specific patients to determine optimal treatment. Outfitted with digital scanners and internet access, any clinic could offer such capabilities, enabling global access to therapy personalization.
© 2022. The Author(s).
Conflict of interest statement
A.E., D.v.d.W., and E.C. are employees at Artera. A.E., D.v.d.W., D.N., R.S., and N.N are or were employees of Salesforce.com, Inc. F.Y.F. is an advisor to and holds equity in Artera and is a consultant for Janssen, Roivant, Myovant, Bayer, Novartis, Varian, Blue Earth Diagnostics and Exact Sciences. L.S. received travel support and honorarium from Varian Medical Systems and is on the advisory board for AbbVie. M.K. received funding from Limbus AI, is a consultant for Palette Life Sciences, and is on the advisory board for AbbVie, Ferring, Janssen, and TerSera. A.E.R. is a consultant for Astellas, Bayer, Blue Earth, Janssen, Myovant, Pfizer, Progenics, and Veracyte. H.M.S. is a member of the ASTRO Board and a member of the clinical trials steering committee for Janssen. P.T.T. is a consultant for Johnson & Johnson, RefleXion Medical, Myovant, and AstraZeneca. D.E.S. is a consultant for AstraZeneca, Blue Earth, Bayer, Boston Scientific, Gammatile, Janssen, Novartis, and Varian. The remaining authors declare no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
