

MRI-negative Cushing's Disease: Management Strategy and Outcomes in 15 Cases Utilizing a Pure Endoscopic Endonasal Approach
- PMID: 35676664
- PMCID: PMC9178868
- DOI: 10.1186/s12902-022-01069-5
MRI-negative Cushing's Disease: Management Strategy and Outcomes in 15 Cases Utilizing a Pure Endoscopic Endonasal Approach
Abstract
Background: Cushing's disease (CD) is among the most common etiologies of hypercortisolism. Magnetic resonance imaging (MRI) is often utilized in the diagnosis of CD, however, up to 64% of adrenocorticotropic hormone (ACTH)-producing pituitary microadenomas are undetectable on MRI. We report 15 cases of MRI negative CD who underwent surgical resection utilizing a purely endoscopic endonasal approach.
Methods: Endoscopic endonasal transsphenoidal surgery (EETS) was performed on 134 CD cases by a single surgeon. Fifteen cases met inclusion criteria: no conclusive MRI studies and no previous surgical treatment. Data collected included signs/symptoms, pre- and post-operative hormone levels, and complications resulting from surgical or medical management. Data regarding tumor diameter, location, and tumor residue/recurrence was obtained from both pre- and post-operative MRI. Immunohistochemistry was performed to assess for tumor hormone secretion.
Results: Aside from a statistically significant difference (P = 0.001) in histopathological results between patients with negative and positive MRI, there were no statistically significant difference between these two groups in any other demographic or clinical data point. Inferior petrosal sinus sampling (IPSS) with desmopressin (DDAVP®) administration was performed on the 15 patients with inconclusive MRIs to identify the origin of ACTH hypersecretion via a central/peripheral (C/P) ratio. IPSS in seven, five and three patients showed right, left, and central side lateralization, respectively. With a mean follow-up of 5.5 years, among MRI-negative patients, 14 (93%) and 12 patients (80%) achieved early and long-term remission, respectively. In the MRI-positive cohort, over a mean follow-up of 4.8 years, 113 patients (94.9%) and 102 patients (85.7%) achieved initial and long-term remission, respectively.
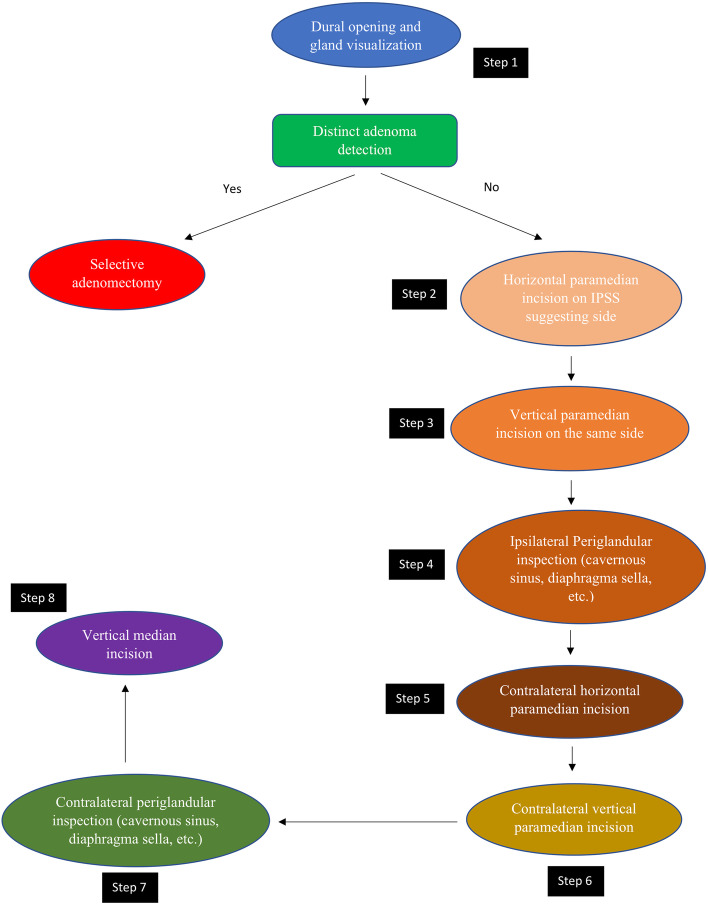
Conclusions: Surgical management of MRI-negative/inconclusive Cushing's disease is challenging scenario requiring a multidisciplinary approach. An experienced neurosurgeon, in collaboration with a dedicated endocrinologist, should identify the most likely location of the adenoma utilizing IPSS findings, followed by careful surgical exploration of the pituitary to identify the adenoma.
Keywords: Cushing’s disease; Endoscopic transsphenoidal surgery; Management; Negative MRI; Outcome.
© 2022. The Author(s).
Conflict of interest statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
