

Nanosensitizers for sonodynamic therapy for glioblastoma multiforme: current progress and future perspectives
- PMID: 35676737
- PMCID: PMC9178901
- DOI: 10.1186/s40779-022-00386-z
Nanosensitizers for sonodynamic therapy for glioblastoma multiforme: current progress and future perspectives
Abstract
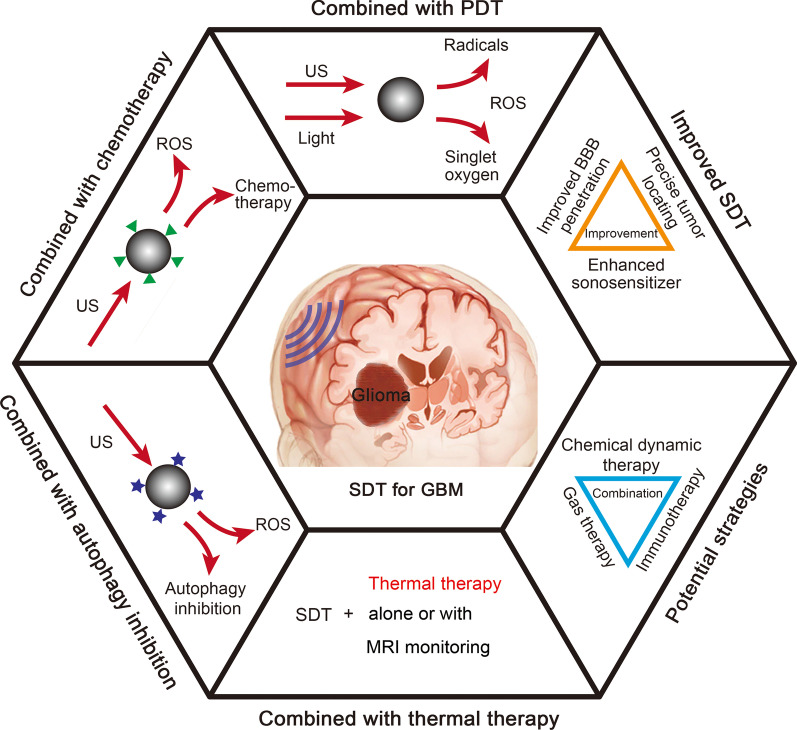
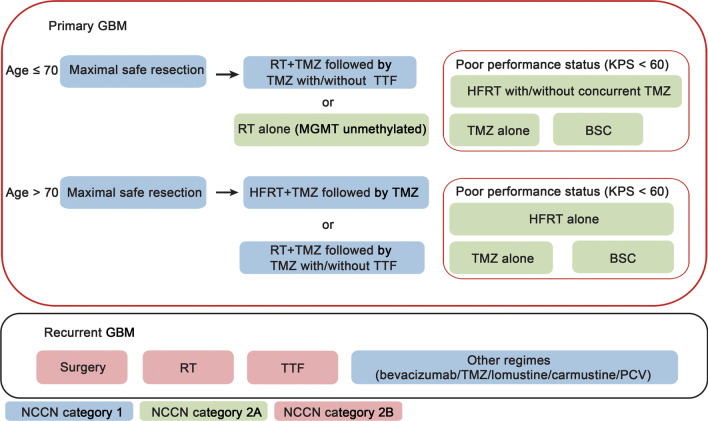
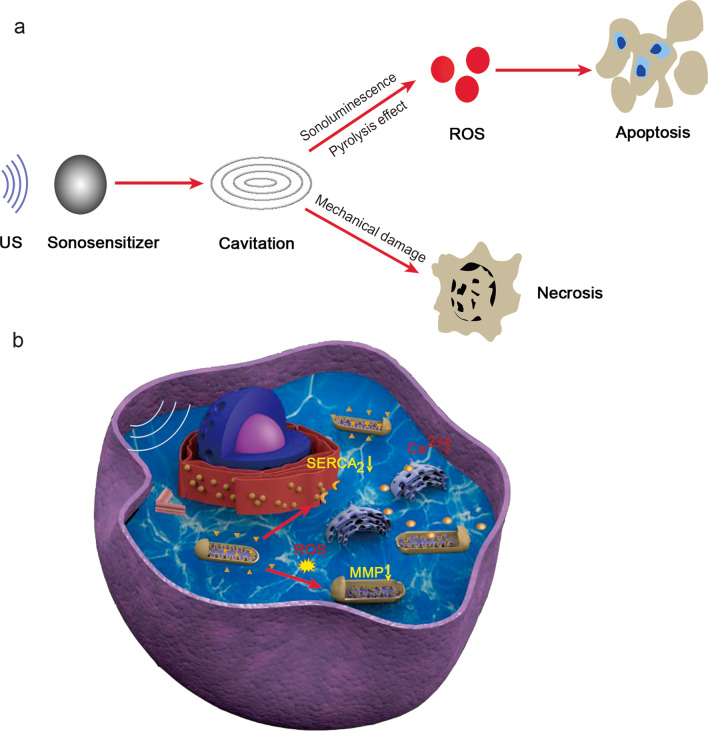
Glioblastoma multiforme (GBM) is the most common primary malignant brain tumor, and it is associated with poor prognosis. Its characteristics of being highly invasive and undergoing heterogeneous genetic mutation, as well as the presence of the blood-brain barrier (BBB), have reduced the efficacy of GBM treatment. The emergence of a novel therapeutic method, namely, sonodynamic therapy (SDT), provides a promising strategy for eradicating tumors via activated sonosensitizers coupled with low-intensity ultrasound. SDT can provide tumor killing effects for deep-seated tumors, such as brain tumors. However, conventional sonosensitizers cannot effectively reach the tumor region and kill additional tumor cells, especially brain tumor cells. Efforts should be made to develop a method to help therapeutic agents pass through the BBB and accumulate in brain tumors. With the development of novel multifunctional nanosensitizers and newly emerging combination strategies, the killing ability and selectivity of SDT have greatly improved and are accompanied with fewer side effects. In this review, we systematically summarize the findings of previous studies on SDT for GBM, with a focus on recent developments and promising directions for future research.
Keywords: Blood–brain barrier (BBB); Combination therapy; Glioblastoma multiforme (GBM); Sonodynamic therapy (SDT); Sonosensitizers.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Ringel F, Pape H, Sabel M, Krex D, Bock HC, Misch M, et al. Clinical benefit from resection of recurrent glioblastomas: results of a multicenter study including 503 patients with recurrent glioblastomas undergoing surgical resection. Neuro Oncol. 2015;18(1):96–104. doi: 10.1093/neuonc/nov145. - DOI - PMC - PubMed
-
- Nayak L, Molinaro AM, Peters K, Clarke JL, Jordan JT, de Groot J, et al. Randomized phase II and biomarker study of pembrolizumab plus bevacizumab versus pembrolizumab alone for patients with recurrent glioblastoma. Clin Cancer Res. 2021;27(4):1048–1057. doi: 10.1158/1078-0432.CCR-20-2500. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
