

Hospital costs associated with adverse events in people with diabetes in the UK
- PMID: 35676793
- PMCID: PMC9796307
- DOI: 10.1111/dom.14796
Hospital costs associated with adverse events in people with diabetes in the UK
Abstract
Aim: To estimate the annual hospital costs associated with a range of adverse events for people with diabetes in the UK.
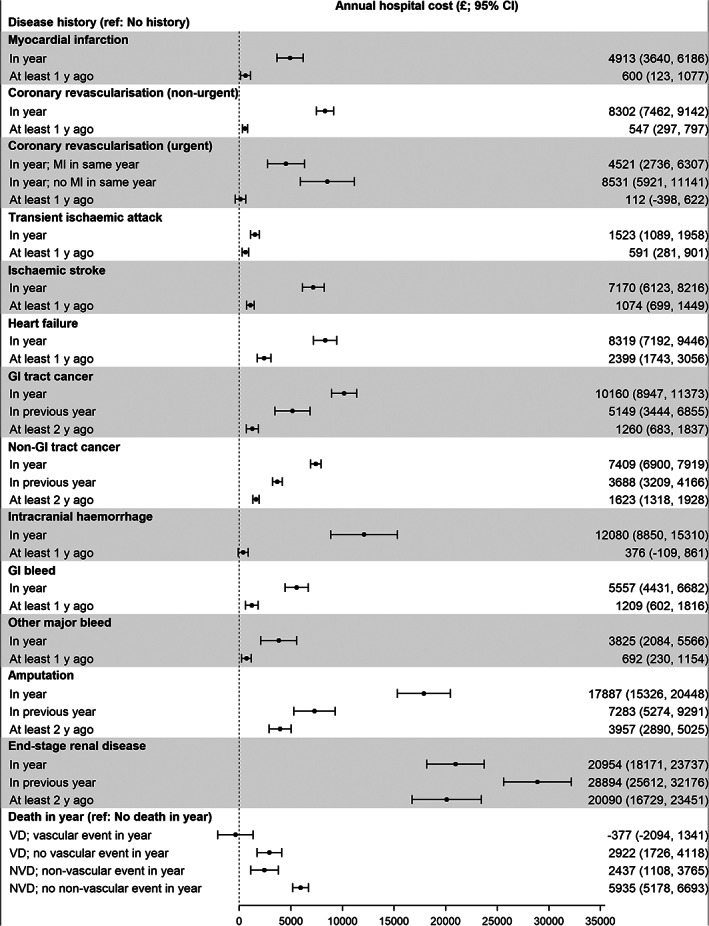
Methods: Annual hospital costs (2019/2020) were derived from 15 436 ASCEND participants from 2005 to 2017 (120 420 person-years). The annual hospital costs associated with cardiovascular events (myocardial infarction, coronary revascularization, transient ischaemic attack [TIA], ischaemic stroke, heart failure), bleeding (gastrointestinal [GI] bleed, intracranial haemorrhage, other major bleed), cancer (GI tract cancer, non-GI tract cancer), end-stage renal disease (ESRD), lower limb amputation and death (vascular, non-vascular) were estimated using a generalized linear model following adjustment for participants' sociodemographic and clinical factors.
Results: In the year of event, ESRD was associated with the largest increase in annual hospital cost (£20 954), followed by lower limb amputation (£17 887), intracranial haemorrhage (£12 080), GI tract cancer (£10 160), coronary revascularization (£8531 if urgent; £8302 if non-urgent), heart failure (£8319), non-GI tract cancer (£7409), ischaemic stroke (£7170), GI bleed (£5557), myocardial infarction (£4913), other major bleed (£3825) and TIA (£1523). In subsequent years, most adverse events were associated with lasting but smaller increases in hospital costs, except for ESRD, where the additional cost remained high (£20 090).
Conclusions: Our study provides robust estimates of annual hospital costs associated with a range of adverse events in people with diabetes that can inform future cost-effectiveness analyses of diabetes interventions. It also highlights the potential cost savings that could be derived from prevention of these costly complications.
Keywords: cardiovascular disease; cost-effectiveness; diabetes complications; health economics.
© 2022 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
All authors declare no conflict of interests relevant to this article.
Figures

References
-
- Beaudet A, Clegg J, Thuresson PO, Lloyd A, McEwan P. Review of utility values for economic modeling in type 2 diabetes. Value Health. 2014;17(4):462‐470. - PubMed
-
- Hayes A, Arima H, Woodward M, et al. Changes in quality of life associated with complications of diabetes: results from the ADVANCE study. Value Health. 2016;19(1):36‐41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
