

Primary Hepatoid Adenocarcinoma of the Lung: A Systematic Literature Review
- PMID: 35676912
- PMCID: PMC9167841
- DOI: 10.2147/OTT.S364465
Primary Hepatoid Adenocarcinoma of the Lung: A Systematic Literature Review
Abstract
Background: Hepatoid adenocarcinoma (HAC) of the lung (HAL) is a rare and aggressive extrahepatic adenocarcinoma with an unknown etiology and unfavorable prognosis, which is similar to the pathophysiological characteristics of hepatocellular carcinoma (HCC).
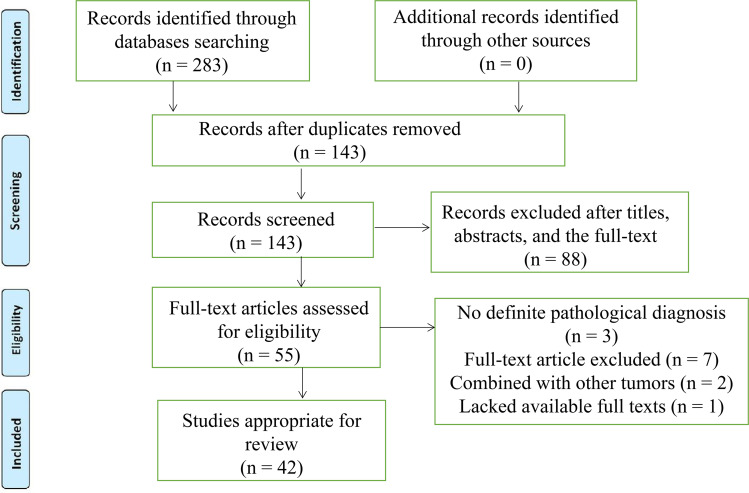
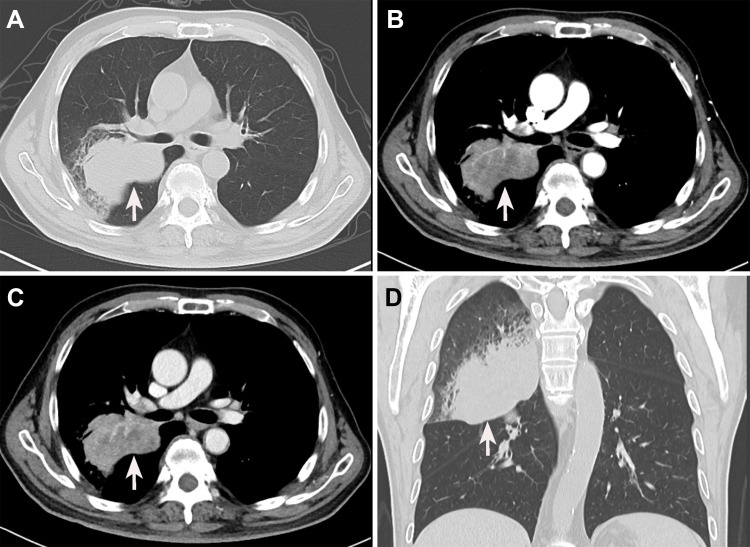
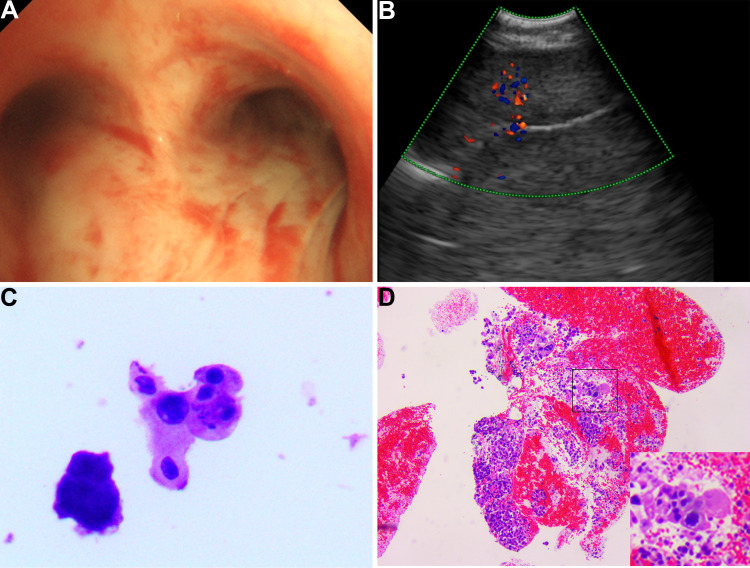
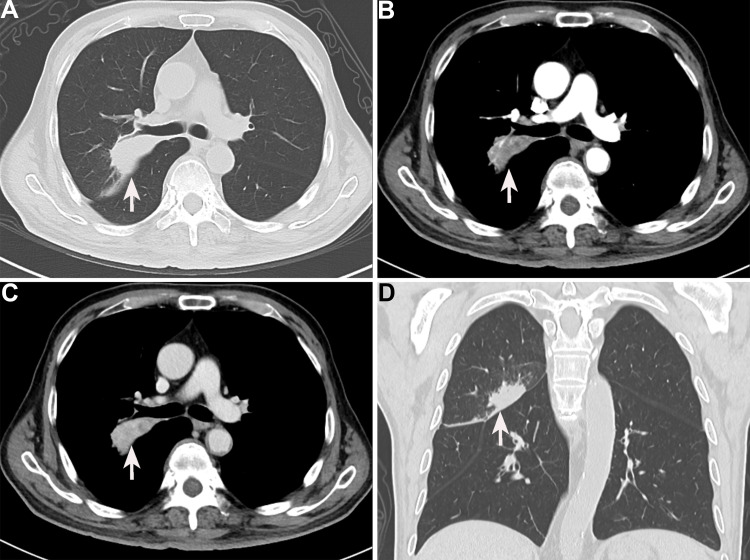
Methods: We first presented a 67-year-old patient diagnosed with HAC in the right middle lobe of the lung. Then, a systematic literature search was performed for HAL cases recorded between 1990 and 2020 based on three databases. The clinicopathological features, therapeutic method, and prognosis of this rare disease were reviewed, and corresponding prognostic factors were explored using Kaplan-Meier (K-M) curve and Cox proportional hazards regression model. Additionally, the potential biological mechanisms of HAL were further explored and compared with HCC and lung adenocarcinoma (LUAD) based on online databases.
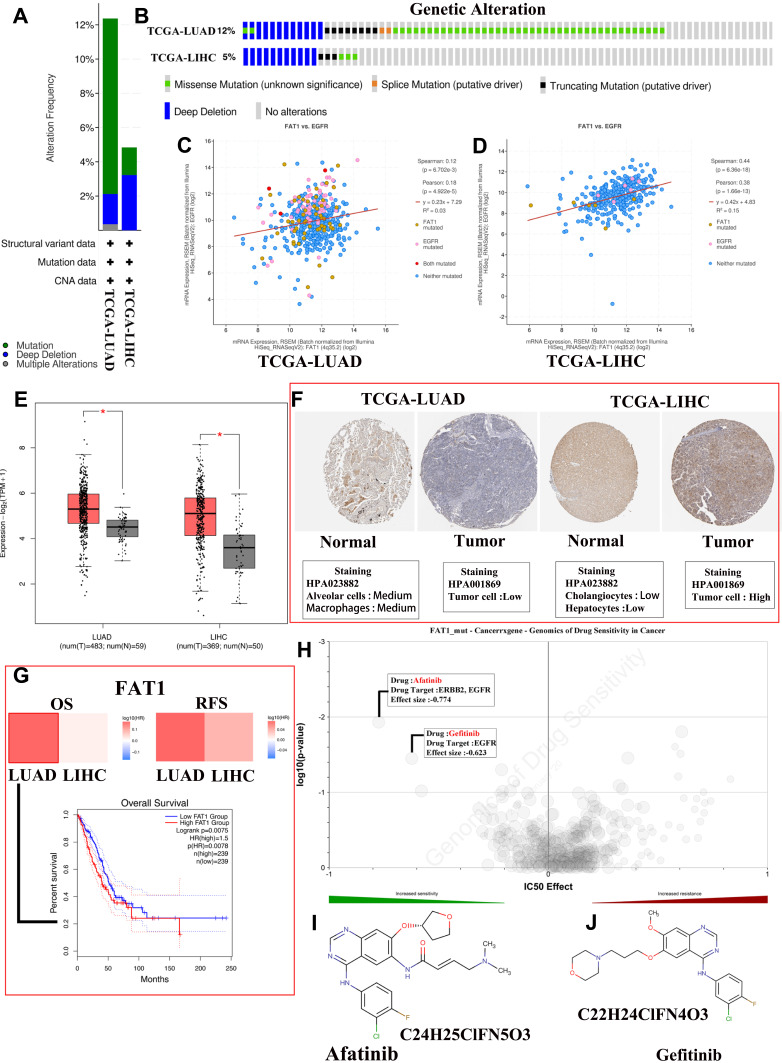
Results: In the present study, we reported an HAL patient who underwent surgical resection combined with chemotherapy and succumbed to disease 13 months after surgery. Additionally, a total of 43 experimental studies with 49 HAL patients, including the present case, met the inclusion criteria and were included in the present review. We found that HAL is characterized by a male-dominated incidence and is more common in the right lung. Patients in the surgical subgroup have a better prognosis than those in the non-surgical subgroup (p = 0.034). Moreover, the Cox proportional hazards regression model demonstrated that surgical resection can significantly improve the prognosis of HAL patients (p = 0.016). HAL is a rare disease associated with gene mutations that has a distinctive cause and unique pathogenesis. Additionally, Afatinib and Gefitinib may be new effective agents to better combat HAL.
Conclusion: In conclusion, males may exhibit an increased risk of developing HAL and poorer prognosis than females. Surgical resection combined with chemotherapy may prolong the survival of patients with HAL. HAL has its unique clinicopathological characteristics and biological mechanisms.
Keywords: HAL; biological mechanisms; hepatoid adenocarcinoma; prognosis; review.
© 2022 Chen et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Comment in
-
Hepatoid Adenocarcinoma of the Lung: Beyond a Shadow of Doubt and Risk of High Mortality [Letter].Onco Targets Ther. 2022 Aug 2;15:837-838. doi: 10.2147/OTT.S380304. eCollection 2022. Onco Targets Ther. 2022. PMID: 35942190 Free PMC article. No abstract available.
Similar articles
-
Optimal treatment strategies for hepatoid adenocarcinoma of the lung: insights from a comprehensive analysis.BMC Cancer. 2024 Aug 2;24(1):948. doi: 10.1186/s12885-024-12682-z. BMC Cancer. 2024. PMID: 39095810 Free PMC article.
-
Hepatoid Adenocarcinoma of the Lung: A Systematic Review of the Literature From 1981 to 2020.Front Oncol. 2021 Aug 6;11:702216. doi: 10.3389/fonc.2021.702216. eCollection 2021. Front Oncol. 2021. PMID: 34422656 Free PMC article.
-
Clinical characteristics of Hepatoid adenocarcinoma of the lung: Four case reports and literature review.Cancer Treat Res Commun. 2021;29:100474. doi: 10.1016/j.ctarc.2021.100474. Epub 2021 Oct 12. Cancer Treat Res Commun. 2021. PMID: 34656923 Review.
-
Hepatoid Adenocarcinoma of the Lung.Technol Cancer Res Treat. 2021 Jan-Dec;20:15330338211057983. doi: 10.1177/15330338211057983. Technol Cancer Res Treat. 2021. PMID: 34816785 Free PMC article.
-
Clinicopathological features and genomic profiles of hepatoid adenocarcinoma of the lung: Report of four cases.Pathol Res Pract. 2022 Jan;229:153652. doi: 10.1016/j.prp.2021.153652. Epub 2021 Nov 20. Pathol Res Pract. 2022. PMID: 34826742
Cited by
-
Optimal treatment strategies for hepatoid adenocarcinoma of the lung: insights from a comprehensive analysis.BMC Cancer. 2024 Aug 2;24(1):948. doi: 10.1186/s12885-024-12682-z. BMC Cancer. 2024. PMID: 39095810 Free PMC article.
-
A rare case of hepatoid adenocarcinoma of the lung.Clin Respir J. 2023 Dec;17(12):1368-1371. doi: 10.1111/crj.13724. Epub 2023 Dec 10. Clin Respir J. 2023. PMID: 38071759 Free PMC article.
-
Primary hepatoid adenocarcinoma of lung: A rare malignancy mimicking tuberculosis.Lung India. 2023 Nov-Dec;40(6):537-540. doi: 10.4103/lungindia.lungindia_117_23. Lung India. 2023. PMID: 37961962 Free PMC article.
-
Hepatoid Adenocarcinoma of the Lung: A Review of the Most Updated Literature and a Presentation of Three Cases.J Clin Med. 2023 Feb 10;12(4):1411. doi: 10.3390/jcm12041411. J Clin Med. 2023. PMID: 36835946 Free PMC article.
-
A case report of pulmonary hepatoid adenocarcinoma: promoting standardized diagnosis and treatment of the rare disease.Front Immunol. 2023 May 24;14:1203876. doi: 10.3389/fimmu.2023.1203876. eCollection 2023. Front Immunol. 2023. PMID: 37292208 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
