

Role of Traditional Cardiovascular Risk Factors after Initiation of Statin Therapy: A PharmLines Inception Cohort Study
- PMID: 35676913
- PMCID: PMC9155967
- DOI: 10.1155/2022/6587165
Role of Traditional Cardiovascular Risk Factors after Initiation of Statin Therapy: A PharmLines Inception Cohort Study
Abstract
Background: Multiple studies and meta-analyses examined the role of traditional risk factors for cardiovascular events in statin treatment-naive patients. Nowadays, millions receive such therapy for the primary prevention of cardiovascular events (CVE).
Objective: CVEs still occur in patients on primary preventive statin therapy. Therefore, further risk stratification within these patients is urgently needed.
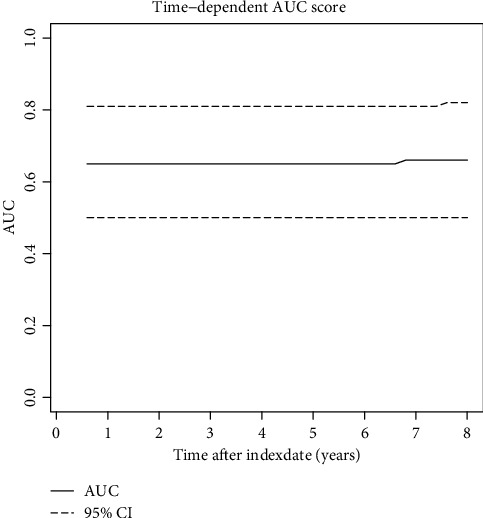
Methods: Using the unique linkage between biomedical data and prescription data from the PharmLines Initiative, we assessed the role of several risk factors used in cardiovascular risk models, using a time-dependent Cox PH model, in the occurrence of drug treatment of CVEs after initiation of statin therapy.
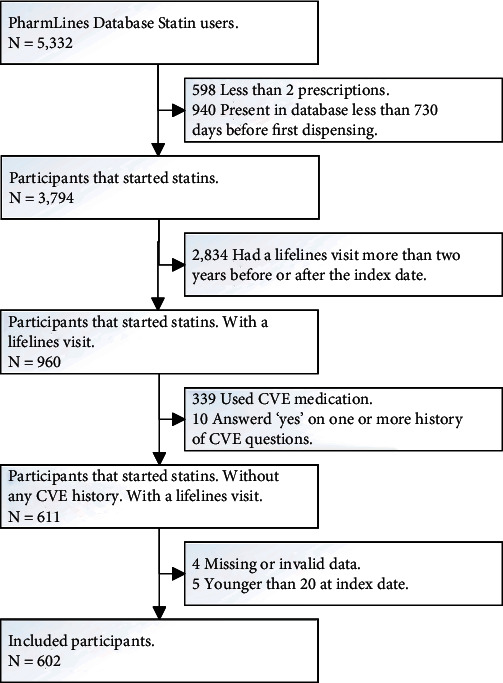
Results: Among 602 statin therapy starters, 11% received drug treatment for CVE within an average follow-up period of 832 days. After multivariable modelling, cholesterol levels and blood pressure at baseline were no longer associated, whereas self-reported diabetes and increasing age were highly associated with the outcome when on statin therapy (hazard ratio (HR): 3.01, 95% confidence interval (95% CI): 1.48-6.12 and 1.04; 95% CI: 1.01-1.07, respectively). Males, smokers, and nonadherent patients had increased risks (HR 1.6, 1.12, and 1.18, resp.), though not statistically significant.
Conclusion: Drug treatment for CVEs after statin initiation is increased in patients with diabetes type 2, in aged patients, males, smokers, and those with poor adherence, while there was no association with baseline cholesterol levels and blood pressure. These factors should be taken into account during the monitoring of statin therapy and may lead to changes in statin treatment or risk-related lifestyle factors.
Copyright © 2022 Dennis Steenhuis et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Relative contributions of statin intensity, achieved low-density lipoprotein cholesterol level, and statin therapy duration to cardiovascular risk reduction in patients with type 2 diabetes: population based cohort study.Cardiovasc Diabetol. 2022 Feb 22;21(1):28. doi: 10.1186/s12933-022-01466-z. Cardiovasc Diabetol. 2022. PMID: 35193571 Free PMC article.
-
Levels and changes of HDL cholesterol and apolipoprotein A-I in relation to risk of cardiovascular events among statin-treated patients: a meta-analysis.Circulation. 2013 Oct 1;128(14):1504-12. doi: 10.1161/CIRCULATIONAHA.113.002670. Epub 2013 Aug 21. Circulation. 2013. PMID: 23965489 Free PMC article.
-
Improving statin treatment strategies to reduce LDL-cholesterol: factors associated with targets' attainment in subjects with and without type 2 diabetes.Cardiovasc Diabetol. 2021 Jul 16;20(1):144. doi: 10.1186/s12933-021-01338-y. Cardiovasc Diabetol. 2021. PMID: 34271920 Free PMC article.
-
Statin-associated incident diabetes: a literature review.Consult Pharm. 2014;29(5):317-34. doi: 10.4140/TCP.n.2014.317. Consult Pharm. 2014. PMID: 24849689 Review.
-
Association of statin use in older people primary prevention group with risk of cardiovascular events and mortality: a systematic review and meta-analysis of observational studies.BMC Med. 2021 Jun 22;19(1):139. doi: 10.1186/s12916-021-02009-1. BMC Med. 2021. PMID: 34154589 Free PMC article.
Cited by
-
Comparative Effectiveness of Anti-Hyperlipidemic Drugs Monotherapy in Primary Prevention of Cardiovascular Disease.Int J Gen Med. 2024 Oct 26;17:4947-4958. doi: 10.2147/IJGM.S479120. eCollection 2024. Int J Gen Med. 2024. PMID: 39478851 Free PMC article.
-
Risk factors for drug-treated major adverse cardio-cerebrovascular events in patients on primary preventive statin therapy: A retrospective cohort study.Prev Med Rep. 2023 May 29;34:102258. doi: 10.1016/j.pmedr.2023.102258. eCollection 2023 Aug. Prev Med Rep. 2023. PMID: 37292425 Free PMC article.
-
The Association between Deductibles and Cardiovascular Medication Adherence: A Retrospective Inception Cohort Study.Drugs Real World Outcomes. 2024 Mar;11(1):99-108. doi: 10.1007/s40801-023-00397-9. Epub 2023 Nov 4. Drugs Real World Outcomes. 2024. PMID: 37925375 Free PMC article.
-
Validation of Medication Proxies for the Identification of Hospitalizations for Major Adverse Cerebro-Cardiovascular Events.Clin Epidemiol. 2025 Mar 28;17:327-336. doi: 10.2147/CLEP.S508754. eCollection 2025. Clin Epidemiol. 2025. PMID: 40171295 Free PMC article.
References
-
- Stichting Pharmaceutische Kengetallen. 25 Miljoen minder aan cholesterolverlagers 2019. 2020. https://www.sfk.nl/publicaties/PW/2019/20ac-25-miljoen-minder-aan-choles... .
-
- Nederlandse Huisartsen Genootschap. Praktische Handleiding bij de NHG-Standaard CVRM (2019) Nederlands: Huisartsen Genootschap; 2019. Mei 2019 ed.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical