

A Pragmatic Approach to Pancreatic Trauma: A Single-Center Experience From a Tertiary Care Center
- PMID: 35677008
- PMCID: PMC9168422
- DOI: 10.7759/cureus.24793
A Pragmatic Approach to Pancreatic Trauma: A Single-Center Experience From a Tertiary Care Center
Abstract
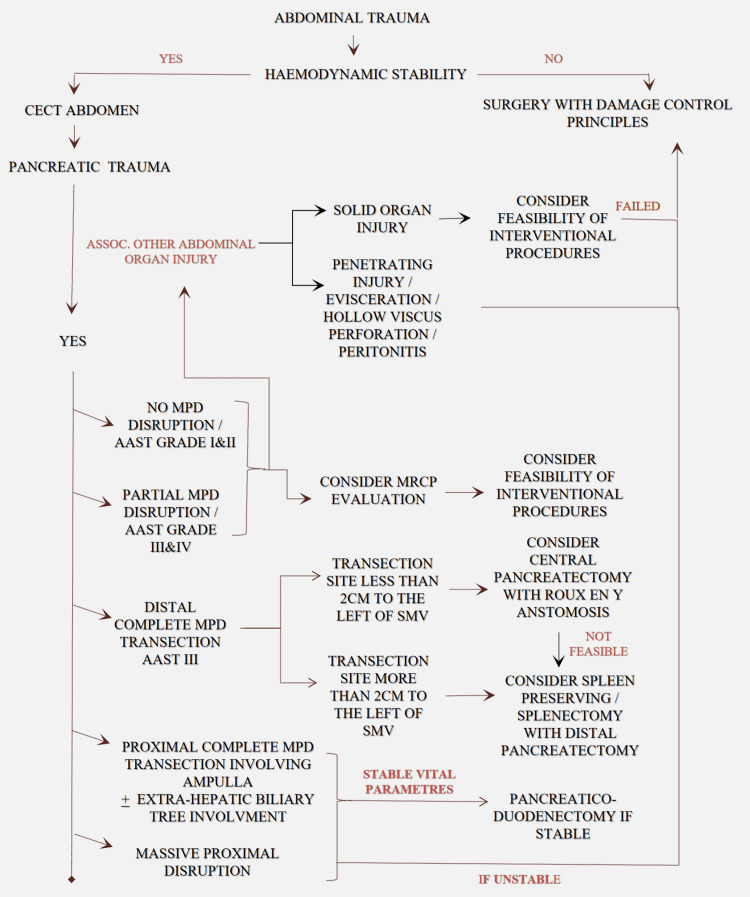
Introduction Pancreatic trauma is rare and is usually associated with adjacent organ and vascular injuries, which adds to the high morbidity and mortality. In the American Association for the Surgery of Trauma (AAST) pancreatic trauma (PT) grading system, the higher grades are a composite of less and more severe extents of injuries. We hereby present an observational study of PT with management based on an indigenous algorithmic approach. Our protocol incorporating both the extent of disruption of the main pancreatic duct (MPD) and its amenability to interventions (endoscopic, radiological, or surgical) is pragmatic. Methods Ours is a retrospective observational study of 28 consecutive cases of PT, done over a three-year period in an academic institution, by an expert Surgical Gastroenterology unit. All patients diagnosed with PT on a contrast abdominal CT scan were included. After stabilization, they were stratified and managed according to an indigenous protocol. The primary outcome measure was treatment success in terms of recovery. The secondary outcome measure was morbidity of any form. Results One patient with Grade 1 PT was operated on for associated hollow viscus injury. Two patients with AAST Grade 2 and two patients with AAST Grade 3 injury were managed successfully without surgery. Twelve of 21 patients with Grade 3 PT underwent Kimura's splenic vessel preserving distal pancreatectomy. Distal pancreatectomy with splenectomy and central pancreatectomy with Roux-en-Y pancreaticojejunostomy (PJ) was done for 7/21 and 2/21 patients, respectively, with Grade 3 PT. Two with Grade 5 injury underwent trauma Whipple. The overall mortality and morbidity rates in our series were 15.7% and 64%, respectively. Conclusion The pathogenesis in PT is a dynamic process and shows temporal evolution. These patients require serial and periodical clinical and radiological monitoring, especially in those managed conservatively initially. PT can be low or high grade. Patients with isolated low-grade PT can be managed according to the standard step-up approach for acute pancreatitis. A carefully selected subgroup of patients with partial MPD disruption either in the head or body of the pancreas can be managed by endotherapy. Complete distal parenchymal transections require early surgery tailored to individual patients in the form of either splenic vessel preserving distal pancreatectomy (SPDP) or distal pancreatectomy with splenectomy (DP+S). Damage control surgery is the dictum in unstable patients with Grades 4 and 5 injuries not responding to resuscitative measures. A trauma Whipple can be done in a carefully selected subgroup of stable patients with proximal massive disruptions in an experienced hepato-pancreatico-biliary (HPB) unit.
Keywords: central pancreatectomy; kimura's procedure; pancreatic trauma; step up approach; whipple's procedure.
Copyright © 2022, Somasekar et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Pancreatic trauma: a ten-year multi-institutional experience. Akhrass R, Yaffe MB, Brandt CP, Reigle M, Fallon WF Jr, Malangoni MA. https://pubmed.ncbi.nlm.nih.gov/9202533/ Am Surg. 1997;63:598–604. - PubMed
-
- Pancreatic trauma - injuries to the pancreas and pancreatic duct. Boffard KD, Brooks AJ. Eur J Surg. 2000;166:4–12. - PubMed
-
- Prognostic factors, morbidity and mortality in pancreatic trauma: a critical appraisal of 432 consecutive patients treated at a level 1 trauma centre. Krige JE, Kotze UK, Setshedi M, Nicol AJ, Navsaria PH. Injury. 2015;46:830–836. - PubMed
-
- The management of pancreatic injuries. Krige J, Jonas E, Thomson S, Beningfield S. Trauma. 2017;19:243–253.
LinkOut - more resources
Full Text Sources
Research Materials