

Encephalopathy in Cirrhosis: Prevention and Management
- PMID: 35677508
- PMCID: PMC9168742
- DOI: 10.1016/j.jceh.2021.12.007
Encephalopathy in Cirrhosis: Prevention and Management
Abstract
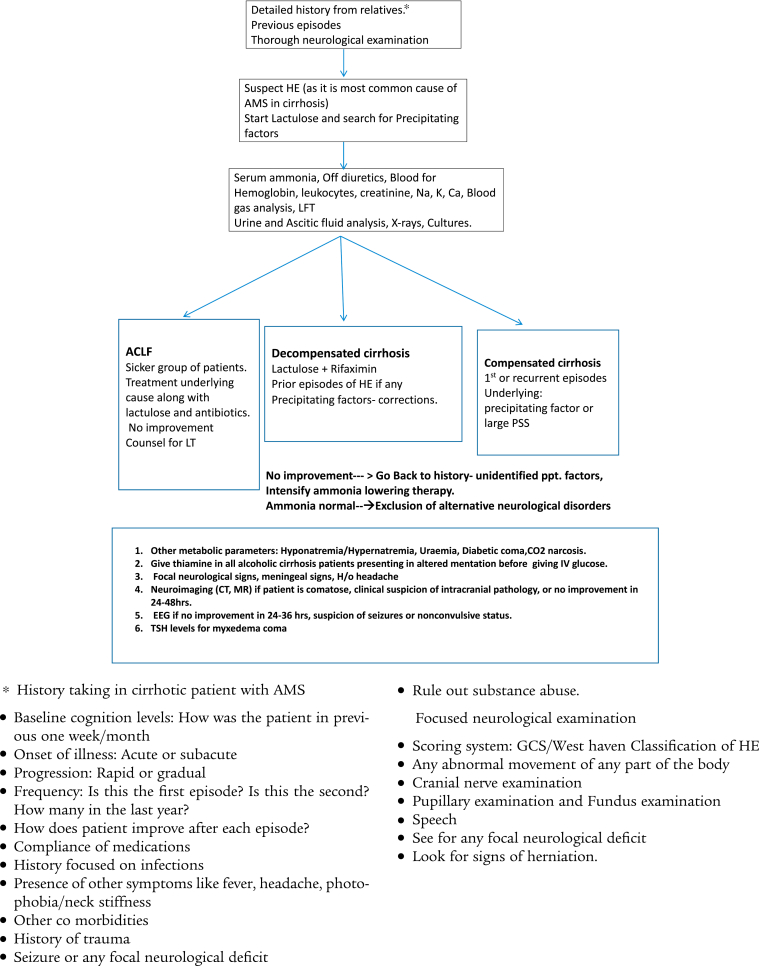
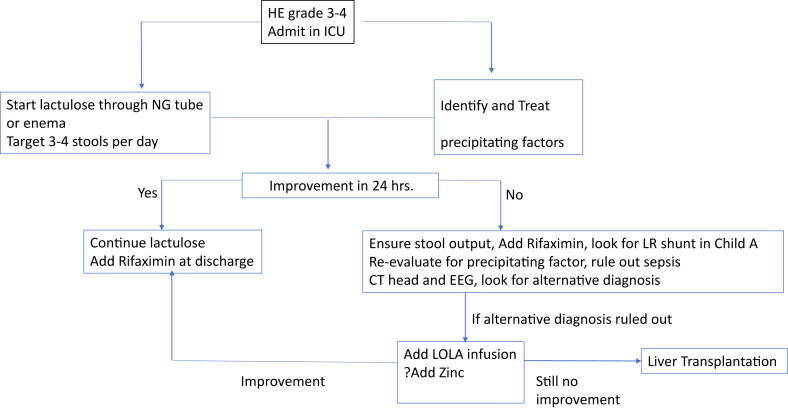
Hepatic encephalopathy (HE) is a major neuropsychiatric complication of cirrhosis. The clinical manifestations of HE ranges from mild confusion, disorientation to altered behaviour and coma in advanced stages. HE is an important cause of recurrent admissions in liver cirrhosis patients. HE is the most common cause of altered mentation in a patient of liver cirrhosis. Lactulose and rifaximin are approved treatment options for the treatment of HE. In patients who have localised neurological signs or are not improving with lactulose and rifaximin should be investigated for other causes of altered sensorium.
Keywords: ALF, Acute Liver Failure; AMS, altered mental state; BCAA, Branched-chain Amino Acids; BRTO, balloon-occluded retrograde transvenous occlusion; CARTO, coil-assisted retrograde transvenous occlusion; FMT; HE, Hepatic encephalopathy; LOLA; OP, Ornithine phenylacetate; PARTO, plug-assisted retrograde transvenous occlusion; SIP, Sickness Impact Profile; cirrhosis; hepatic encephalopathy; lactulose; prevention; probiotics; rifaximin; treatment.
© 2021 Indian National Association for Study of the Liver. Published by Elsevier B.V. All rights reserved.
Figures

References
-
- Ferenci P., Lockwood A., Mullen K., et al. Hepatic encephalopathy—definition, nomenclature, diagnosis, and quantification: final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology. 2002;35:716–721. - PubMed
-
- Amodio P., Del Piccolo F., Pettenò E., et al. Prevalence and prognostic value of quantified electroencephalogram (EEG) alterations in cirrhotic patients. J Hepatol. 2001;35:37–45. - PubMed
-
- Tapper E.B., Halbert B., Mellinger J. Rates of and reasons for hospital readmissions in patients with cirrhosis: a multistate population-based cohort study. Clin Gastroenterol Hepatol. 2016;14:1181–1188.e2. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
