

Aortic dissection-Pulmonary embolism association: A therapeutic dilemma
- PMID: 35677707
- PMCID: PMC9167868
- DOI: 10.1016/j.radcr.2022.04.045
Aortic dissection-Pulmonary embolism association: A therapeutic dilemma
Abstract
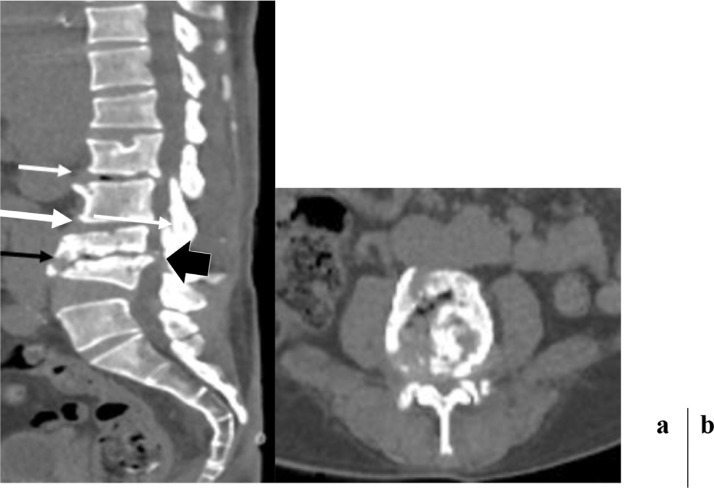
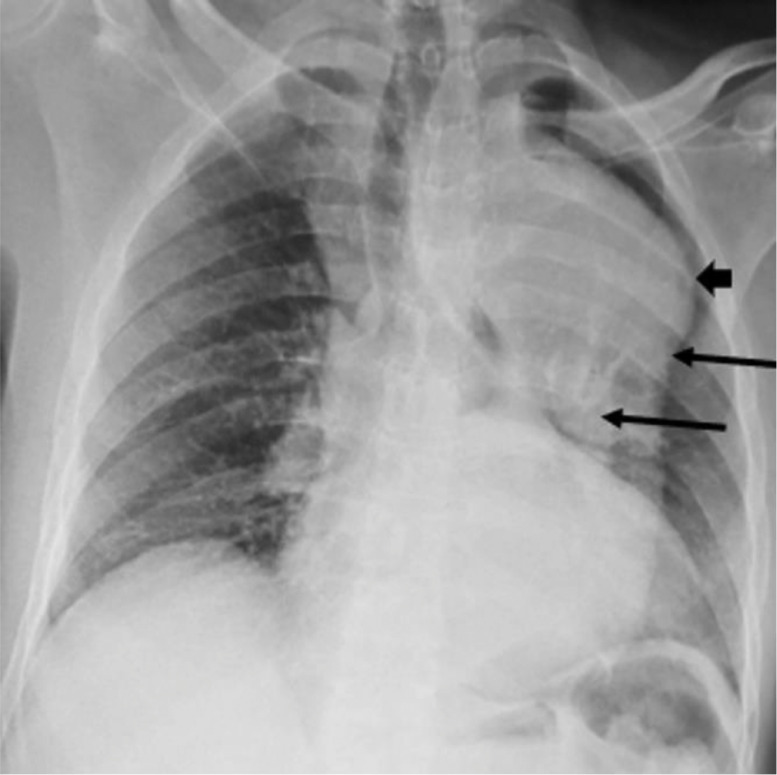
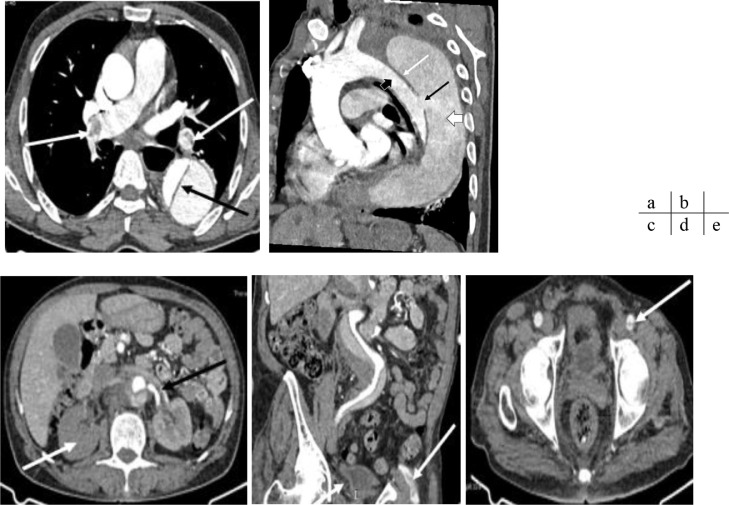
Aortic dissection is a rare but serious condition. Its association with pulmonary embolism is exceptional and produces a real therapeutic dilemma. We are discussing the case of a 67-year-old male patient who presented with paraplegia with infectious syndrome. The chest X-ray performed to screen for an infectious site led to the suspicion of an aortic aneurysm and the CT angiography showed Stanford type B aortic dissection associated with bilateral proximal pulmonary embolism. The treatment was symptomatic and resulted in the patient's death 48 hours after diagnosis. Management of this pathological association is not standardized between establishing anticoagulant therapy and therapeutic abstention. This management depends on the teams and has a very cautious prognosis.
Keywords: Aortic dissection; Pulmonary embolism; Therapeutic dilemma.
© 2022 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures
References
-
- Badidi M, Benyass A, Lakhal Z, Chaib A, Raissouni M, et al. Conduite à tenir devant une dissection aortique aigue. Maroc Méd. 2009;31(3):213–218.
Publication types
LinkOut - more resources
Full Text Sources
