

Save the Greater Trochanter: A Novel Modification to the Extended Trochanteric Osteotomy
- PMID: 35677941
- PMCID: PMC9168376
- DOI: 10.1016/j.artd.2022.05.004
Save the Greater Trochanter: A Novel Modification to the Extended Trochanteric Osteotomy
Abstract
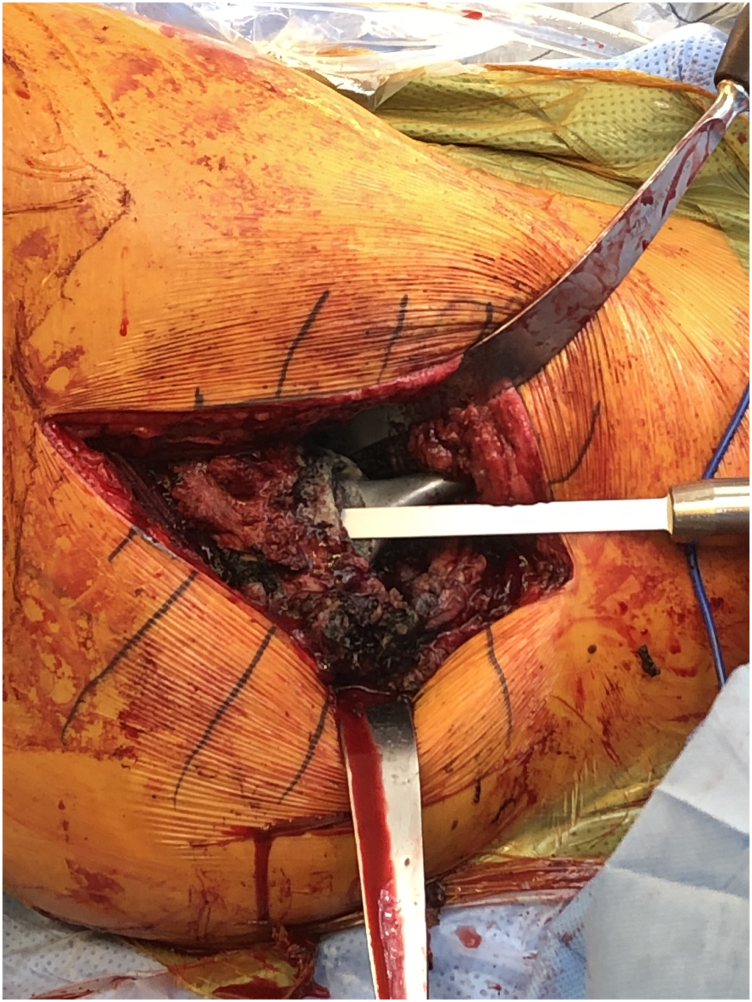
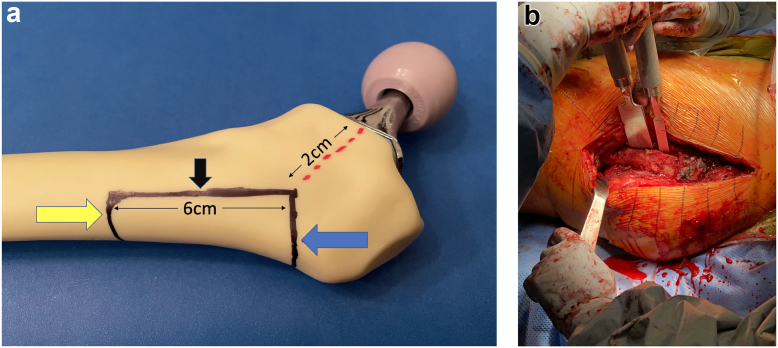
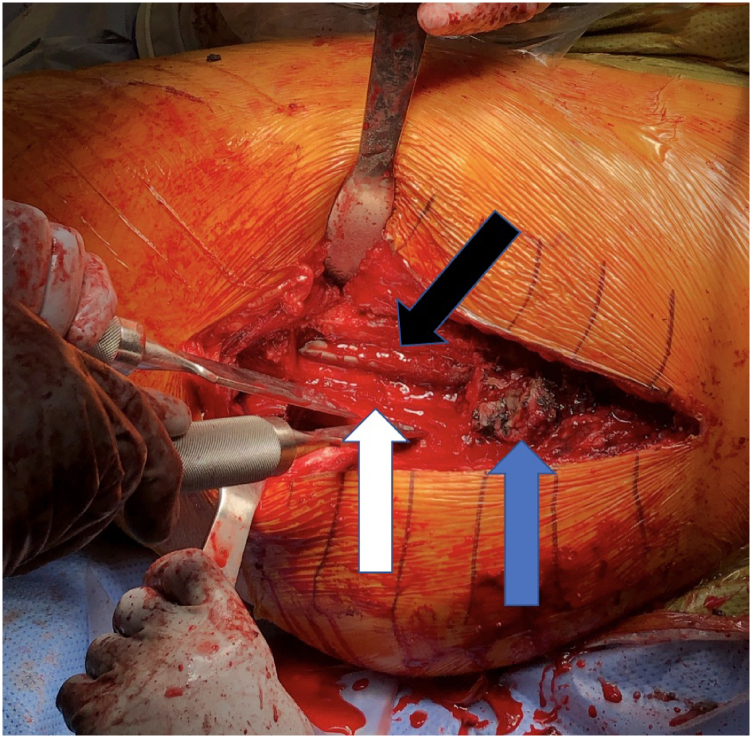
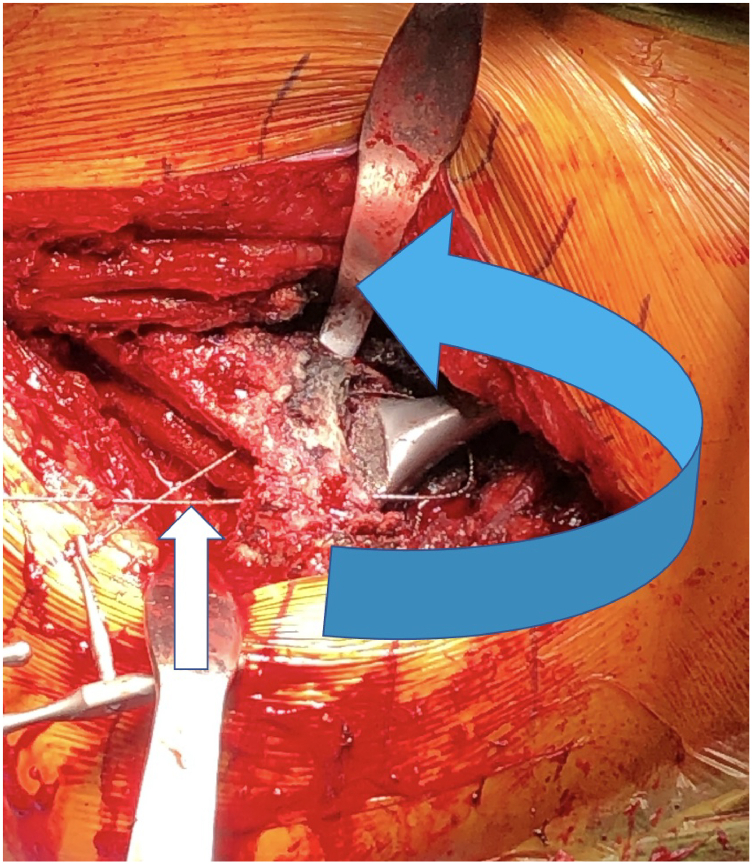
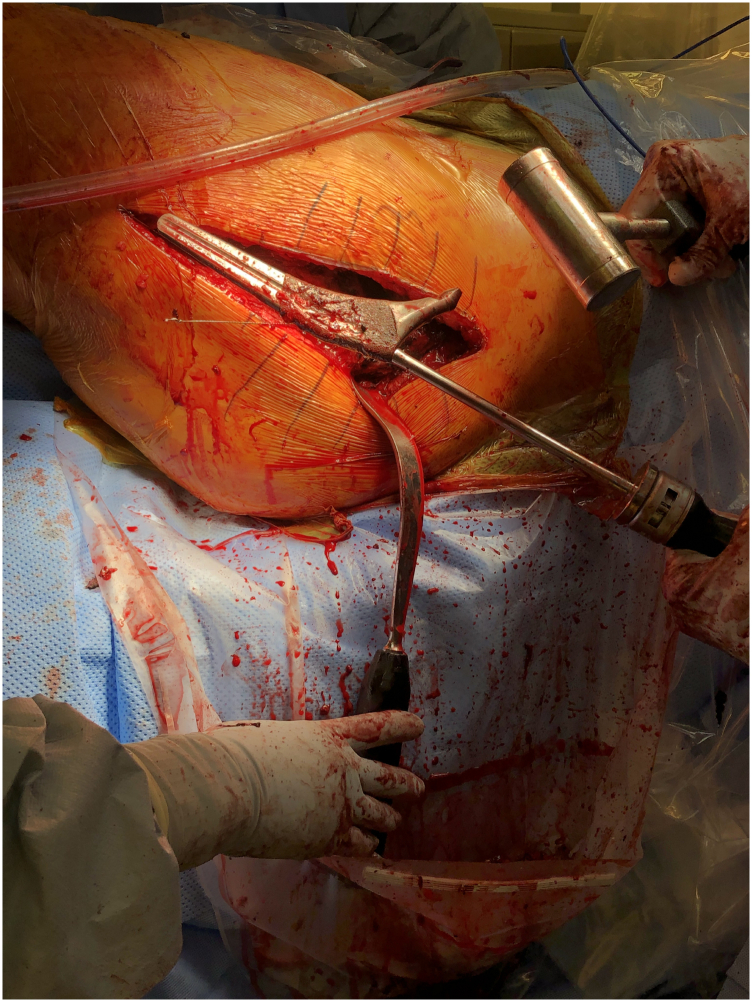
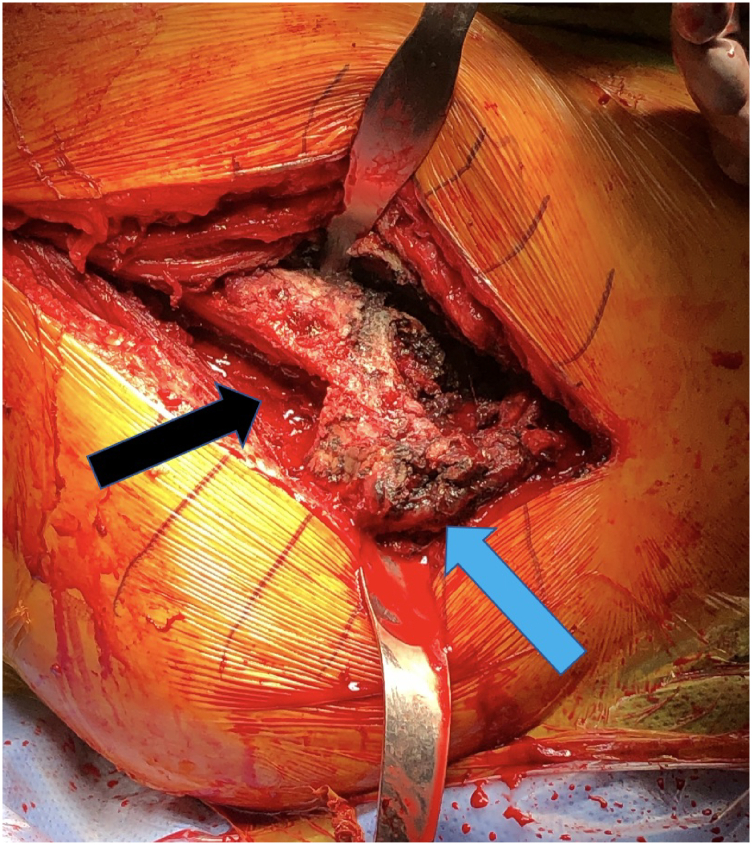
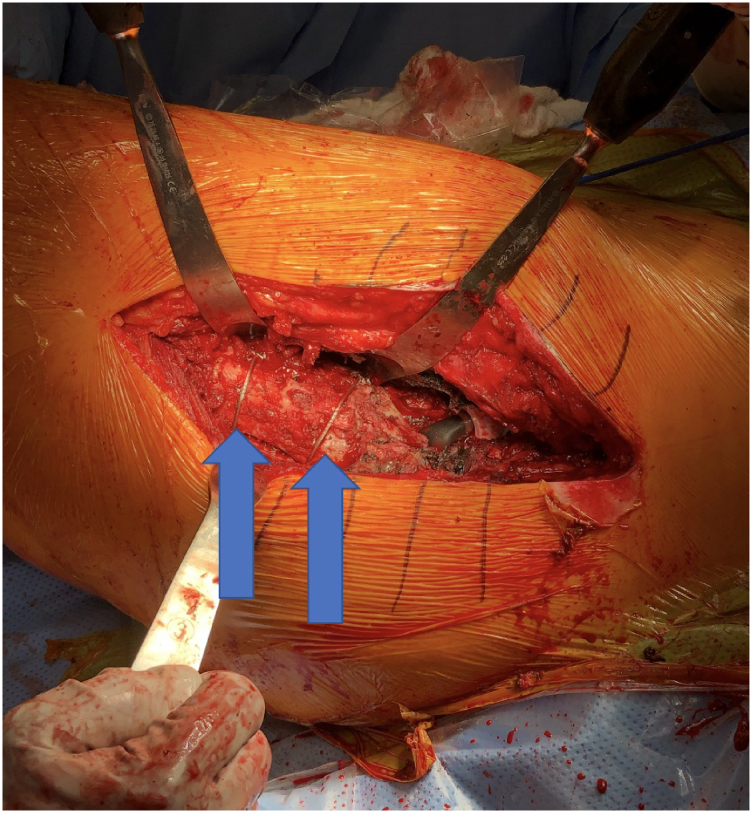
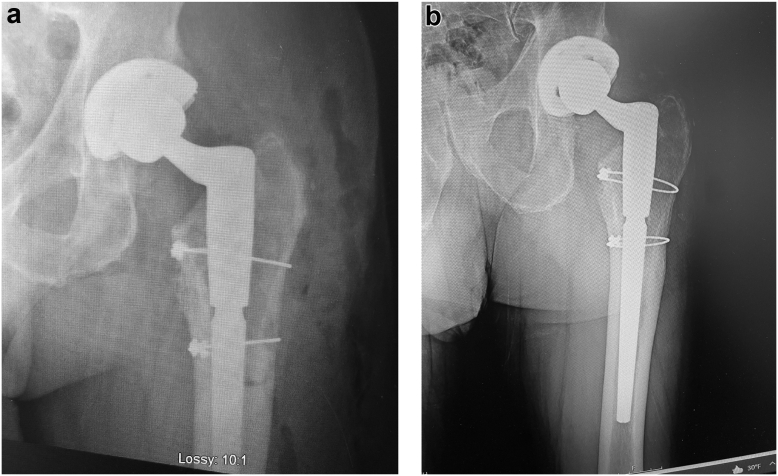
The extended trochanteric osteotomy is the workhorse for removal of well-fixed femoral stems during total hip revision arthroplasty. Despite its reliable performance in exposing the implants for removal and accessing the femoral canal, significant complications can occur. Though these complications are rare, trochanteric nonunion, trochanteric escape, and femoral implant subsidence can have a significant negative impact on gait mechanics and patient outcome. If access to the canal was still possible and the greater trochanter could remain in place, these complications could be minimized or possibly even eliminated. This paper describes a novel technique using a lateral cortical window just distal to the greater trochanter that allows removal of a well-fixed stem and leaves the greater trochanter intact.
Keywords: Extended trochanteric osteotomy; Femoral stem removal; Surgical technique; Total hip revision.
© 2022 The Authors.
Figures

References
-
- Lerch M., von Lewinski G., Windhagen H., Thorey F. Revision of total hip arthroplasty: clinical outcome of extended trochanteric osteotomy and intraoperative femoral fracture. Technol Health Care. 2008;16:293–300. - PubMed
-
- Mardones R., Gonzalez C., Cabanela M.E., Trousdale R.T., Berry D.J. Extended femoral osteotomy for revision of hip arthroplasty: results and complications. J Arthroplasty. 2005;20:79–83. - PubMed
-
- Park Y.S., Moon Y.W., Lim S.J. Revision total hip arthroplasty using a fluted and tapered modular distal fixation stem with and without extended trochanteric osteotomy. J Arthroplasty. 2007;22:993–999. - PubMed
-
- MacDonald S.J., Cole C., Guerin J., Rorabeck C.H., Bourne R.B., McCalden R.W. Extended trochanteric osteotomy via the direct lateral approach in revision hip arthroplasty. Clin Orthop Relat Res. 2003;417:210–216. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
