

Etiology, 3-Month Functional Outcome and Recurrent Events in Non-Traumatic Intracerebral Hemorrhage
- PMID: 35677981
- PMCID: PMC9194537
- DOI: 10.5853/jos.2021.01823
Etiology, 3-Month Functional Outcome and Recurrent Events in Non-Traumatic Intracerebral Hemorrhage
Abstract
Background and purpose: Knowledge about different etiologies of non-traumatic intracerebral hemorrhage (ICH) and their outcomes is scarce.
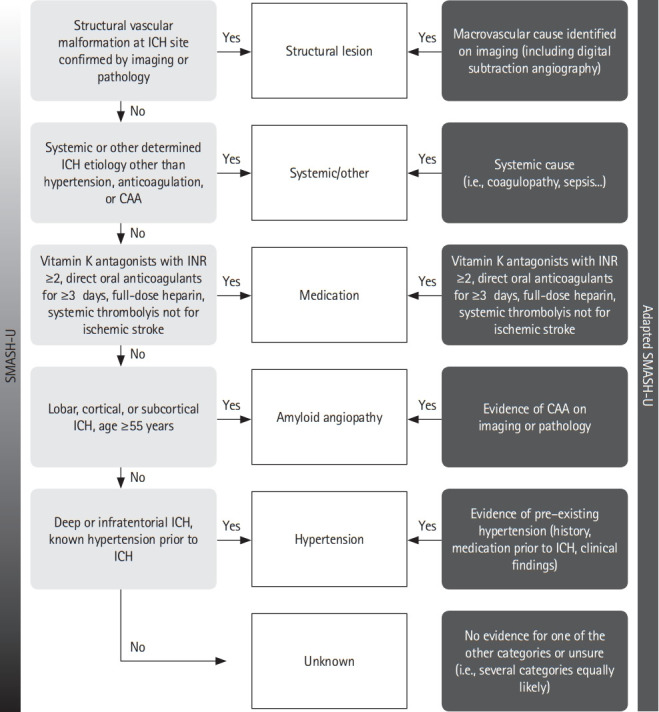
Methods: We assessed prevalence of pre-specified ICH etiologies and their association with outcomes in consecutive ICH patients enrolled in the prospective Swiss Stroke Registry (2014 to 2019).
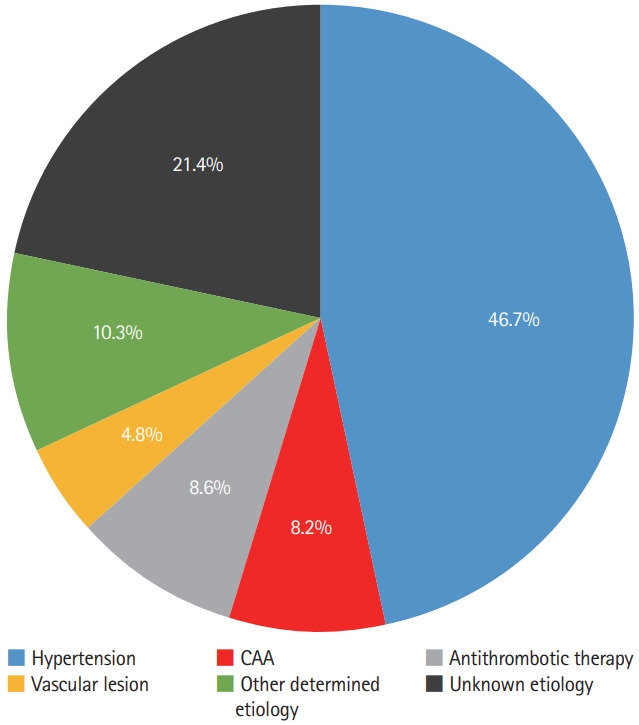
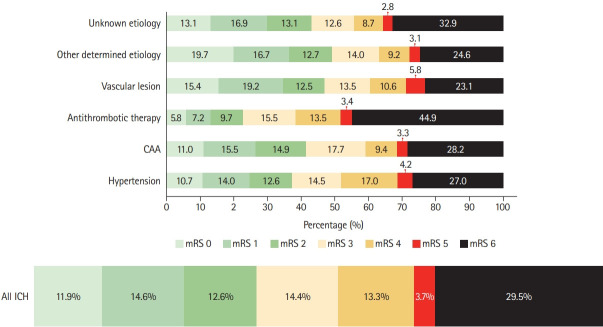
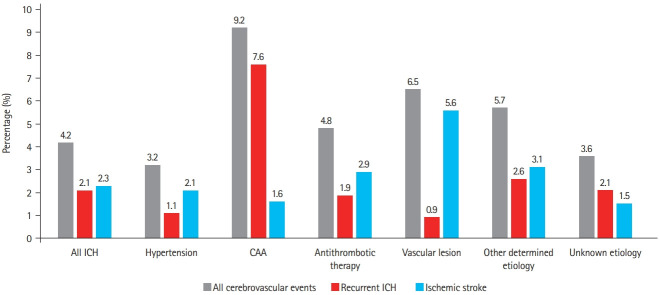
Results: We included 2,650 patients (mean±standard deviation age 72±14 years, 46.5% female, median National Institutes of Health Stroke Scale 8 [interquartile range, 3 to 15]). Etiology was as follows: hypertension, 1,238 (46.7%); unknown, 566 (21.4%); antithrombotic therapy, 227 (8.6%); cerebral amyloid angiopathy (CAA), 217 (8.2%); macrovascular cause, 128 (4.8%); other determined etiology, 274 patients (10.3%). At 3 months, 880 patients (33.2%) were functionally independent and 664 had died (25.1%). ICH due to hypertension had a higher odds of functional independence (adjusted odds ratio [aOR], 1.33; 95% confidence interval [CI], 1.00 to 1.77; P=0.05) and lower mortality (aOR, 0.64; 95% CI, 0.47 to 0.86; P=0.003). ICH due to antithrombotic therapy had higher mortality (aOR, 1.62; 95% CI, 1.01 to 2.61; P=0.045). Within 3 months, 4.2% of patients had cerebrovascular events. The rate of ischemic stroke was higher than that of recurrent ICH in all etiologies but CAA and unknown etiology. CAA had high odds of recurrent ICH (aOR, 3.38; 95% CI, 1.48 to 7.69; P=0.004) while the odds was lower in ICH due to hypertension (aOR, 0.42; 95% CI, 0.19 to 0.93; P=0.031).
Conclusions: Although hypertension is the leading etiology of ICH, other etiologies are frequent. One-third of ICH patients are functionally independent at 3 months. Except for patients with presumed CAA, the risk of ischemic stroke within 3 months of ICH was higher than the risk of recurrent hemorrhage.
Keywords: Cerebral hemorrhage; Etiology; Ischemic stroke; Outcome.
Figures

References
-
- Cordonnier C, Demchuk A, Ziai W, Anderson CS. Intracerebral haemorrhage: current approaches to acute management. Lancet. 2018;392:1257–1268. - PubMed
-
- Hostettler IC, Seiffge DJ, Werring DJ. Intracerebral hemorrhage: an update on diagnosis and treatment. Expert Rev Neurother. 2019;19:679–694. - PubMed
-
- Shoamanesh A, Patrice Lindsay M, Castellucci LA, Cayley A, Crowther M, de Wit K, et al. Canadian stroke best practice recommendations: management of spontaneous intracerebral hemorrhage, 7th edition update 2020. Int J Stroke. 2021;16:321–341. - PubMed
-
- Steiner T, Al-Shahi Salman R, Beer R, Christensen H, Cordonnier C, Csiba L, et al. European Stroke Organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage. Int J Stroke. 2014;9:840–855. - PubMed
-
- Adams HP, Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, et al. Classification of subtype of acute ischemic stroke: definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993;24:35–41. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
