

Interventions for treating supracondylar elbow fractures in children
- PMID: 35678077
- PMCID: PMC9178297
- DOI: 10.1002/14651858.CD013609.pub2
Interventions for treating supracondylar elbow fractures in children
Abstract
Background: Elbow supracondylar fractures are common, with treatment decisions based on fracture displacement. However, there remains controversy regarding the best treatments for this injury.
Objectives: To assess the effects (benefits and harms) of interventions for treating supracondylar elbow fractures in children.
Search methods: We searched CENTRAL, MEDLINE, and Embase in March 2021. We also searched trial registers and reference lists. We applied no language or publication restrictions.
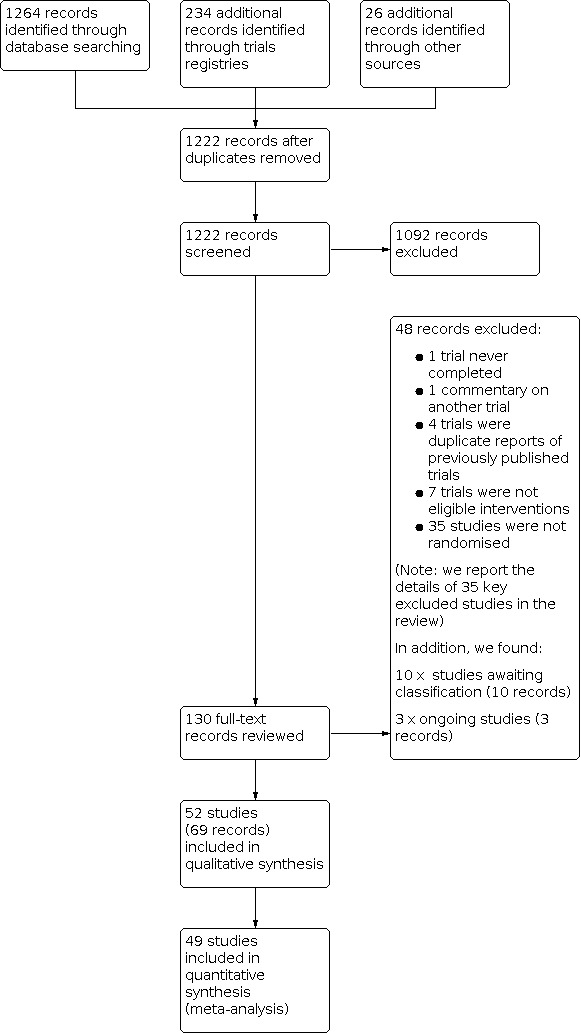
Selection criteria: We included randomised and quasi-randomised controlled trials comparing different interventions for the treatment of supracondylar elbow fractures in children. We included studies investigating surgical interventions (different fixation techniques and different reduction techniques), surgical versus non-surgical treatment, traction types, methods of non-surgical intervention, and timing and location of treatment.
Data collection and analysis: We used standard methodological procedures expected by Cochrane. We collected data and conducted GRADE assessment for five critical outcomes: functional outcomes, treatment failure (requiring re-intervention), nerve injury, major complications (pin site infection in most studies), and cosmetic deformity (cubitus varus). MAIN RESULTS: We included 52 trials with 3594 children who had supracondylar elbow fractures; most were Gartland 2 and 3 fractures. The mean ages of children ranged from 4.9 to 8.4 years and the majority of participants were boys. Most studies (33) were conducted in countries in South-East Asia. We identified 12 different comparisons of interventions: retrograde lateral wires versus retrograde crossed wires; lateral crossed (Dorgan) wires versus retrograde crossed wires; retrograde lateral wires versus lateral crossed (Dorgan) wires; retrograde crossed wires versus posterior intrafocal wires; retrograde lateral wires in a parallel versus divergent configuration; retrograde crossed wires using a mini-open technique or inserted percutaneously; buried versus non-buried wires; external versus internal fixation; open versus closed reduction; surgical fixation versus non-surgical immobilisation; skeletal versus skin traction; and collar and cuff versus backslab. We report here the findings of four comparisons that represent the most substantial body of evidence for the most clinically relevant comparisons. All studies in these four comparisons had unclear risks of bias in at least one domain. We downgraded the certainty of all outcomes for serious risks of bias, for imprecision when evidence was derived from a small sample size or had a wide confidence interval (CI) that included the possibility of benefits or harms for both treatments, and when we detected the possibility of publication bias. Retrograde lateral wires versus retrograde crossed wires (29 studies, 2068 children) There was low-certainty evidence of less nerve injury with retrograde lateral wires (RR 0.65, 95% CI 0.46 to 0.90; 28 studies, 1653 children). In a post hoc subgroup analysis, we noted a greater difference in the number of children with nerve injuries when lateral wires were compared to crossed wires inserted with a percutaneous medial wire technique (RR 0.41, 95% CI 0.20 to 0.81, favours lateral wires; 10 studies, 552 children), but little difference when an open technique was used (RR 0.91, 95% CI 0.59 to 1.40, favours lateral wires; 11 studies, 656 children). Although we noted a statistically significant difference between these subgroups from the interaction test (P = 0.05), we could not rule out the possibility that other factors could account for this difference. We found little or no difference between the interventions in major complications, which were described as pin site infections in all studies (RR 1.08, 95% CI 0.65 to 1.79; 19 studies, 1126 children; low-certainty evidence). For functional status (1 study, 35 children), treatment failure requiring re-intervention (1 study, 60 children), and cosmetic deformity (2 studies, 95 children), there was very low-certainty evidence showing no evidence of a difference between interventions. Open reduction versus closed reduction (4 studies, 295 children) Type of reduction method may make little or no difference to nerve injuries (RR 0.30, 95% CI 0.09 to 1.01, favours open reduction; 3 studies, 163 children). However, there may be fewer major complications (pin site infections) when closed reduction is used (RR 4.15, 95% CI 1.07 to 16.20; 4 studies, 253 children). The certainty of the evidence for these outcomes is low. No studies reported functional outcome, treatment failure requiring re-intervention, or cosmetic deformity. The four studies in this comparison used direct visualisation during surgery. One additional study used a joystick technique for reduction, and we did not combine data from this study in analyses. Surgical fixation using wires versus non-surgical immobilisation using a cast (3 studies, 140 children) There was very low-certainty evidence showing little or no difference between interventions for treatment failure requiring re-intervention (1 study, 60 children), nerve injury (3 studies, 140 children), major complications (3 studies, 126 children), and cosmetic deformity (2 studies, 80 children). No studies reported functional outcome. Backslab versus sling (1 study, 50 children) No nerve injuries or major complications were experienced by children in either group; this evidence is of very low certainty. Functional outcome, treatment failure, and cosmetic deformity were not reported. AUTHORS' CONCLUSIONS: We found insufficient evidence for many treatments of supracondylar fractures. Fixation of displaced supracondylar fractures with retrograde lateral wires compared with crossed wires provided the most substantial body of evidence in this review, and our findings indicate that there may be a lower risk of nerve injury with retrograde lateral wires. In future trials of treatments, we would encourage the adoption of a core outcome set, which includes patient-reported measures. Evaluation of the effectiveness of traction compared with surgical fixation would provide a valuable addition to this clinical field.
Copyright © 2022 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
Ben Marson: none known Adeel Ikram: none known Simon Craxford: none known Kathryn Price: none known Benjamin Ollivere: none known
Figures





































































Update of
References
References to studies included in this review
Abdel Karim 2016 {published data only (unpublished sought but not used)}
-
- Abdel Karim M, Hosny A, Nasef Abdelatif NM, Hegazy MM, Awadallah WR, Khaled SA, et al. Crossed wires versus 2 lateral wires in management of supracondylar fracture of the humerus in children in the hands of junior trainees. Journal of Orthopaedic Trauma 2016;30(4):e123-8. [PMID: ] - PubMed
-
- Hosney A, Abdel Karim M, Mohamadi H. Crossed wires versus two lateral wires in management of supracondylar fracture of the humerus in children. In: American Academy of Orthopaedic Surgeons Annual Meeting: 2014 Mar 11-15; New Orleans (LA). 2014.
Abubeih 2019 {published and unpublished data}
-
- Abubeih HM, El-Adly W, El-Gaafary K, Bakr H. Percutaneous cross-pinning versus two lateral entry pinning in Gartland type III pediatric supracondylar humerus fractures. Egyptian Orthopaedic Journal 2019;54:52-61.
-
- Marson BA. [personal communication]. Email to: HM Abdullah 28 November 2020.
Afaque 2020 {published data only}
-
- Afaque SF, Singh A, Maharjan R, Ranjan R, Panda AK, Mishra A. Comparison of clinic-radiological outcome of cross pinning versus lateral pinning for displaced supracondylar fracture of humerus in children: a randomized controlled trial. Journal of Clinical Orthopaedics and Trauma 2020;11(2):259-63. [PMID: ] - PMC - PubMed
Aher 2018 {published data only}
-
- Aher D, Mishra RK, Gohiya A. Comparative study of two techniques of percutaneous pinning of displaced supracondylar humerus fracture. Orthopaedic Journal of M.P. Chapter 2018;24(1):3-7.
Ahmad 2020 {published data only}
-
- Ahmad MM, Hussain HU, Raza MM, Ahmad S, Iqbal AM, Iqbal U. Comparison of two methods of percutaneous pin fixation in displaced supracondylar fractures of the humerus in children. Medical Journal of South Punjab 2020;1(1):31-5.
Ajmera 2013 {published data only}
-
- Ajmera A, Mukherjee A, Bhargava P, Katare BS, Singh A. Comparison of the percutaneous versus open reduction for displased supracondylar humerus fractures in children. Orthopaedic Journal of MP Chapter 2013;19(2):29-35.
Altay 2011 {published data only}
-
- Altay MA, Erturk C, Altay M, Belhan O, Isikan UE. Ultrasonographic examination of the radial and ulnar nerves after percutaneous cross-wiring of supracondylar humerus fractures in children: a prospective, randomized controlled study. European Journal of Trauma and Emergency Surgery 2011;37(Suppl 1):S101. - PubMed
-
- Altay MA, Erturk C, Altay M, Belhan O, Isikan UE. Ultrasonographic examination of the radial and ulnar nerves after percutaneous cross-wiring of supracondylar humerus fractures in children: a prospective, randomized controlled study. Journal of Pediatric Orthopaedics. Part B 2011;20(5):334-40. [PMID: ] - PubMed
Anwar 2011 {published data only}
-
- Anwar W, Rahman N, Iqbal MJ, Khan MA. Comparison of the two methods of percutaneous K-wire fixation in displaced supracondylar fracture of humerus in children. Journal of Postgraduate Medical Institute 2011;25(4):356-61.
Arun 2018 {published data only}
-
- Arun KN, Ramachandra K, Veerabhadra J, Suman NV, Paila SP, Nagadurga N. A prospective study of crossed versus lateral pinning for displaced extension-type supracondylar fractures of humerus. International Journal of Orthopaedics Sciences 2018;4(4):737-40.
Das 2019 {published data only}
-
- Das S, Santra S, Rahman M, Kar R. The clinical and radiological outcome of percutaneous pinning, in displaced supracondylar fracture of the humerus of children. Journal of the Indian Medical Association 2019;117(10):36-7.
Dawood 2011 {published data only}
-
- Dawood WF. Medial-lateral internal pin fixation compared to 2-lateral internal pin fixation in treatment of completely displaced supracondylar fractures of the humerus in children. Medical Journal of Tikrit University 2011;2(172):61-6.
Dehghan 2012 {published data only (unpublished sought but not used)}
-
- Dehghan M, Bahmani MT. The comparison of two surgical methods of close fixation with pin and open fixation for treatment of supracondylar fracture in under 10 years old patients. Yafte 2012;14(3):67-74.
-
- IRCT201105146480N1. The comparison of two surgery methods for treatment of supracondylar fracture in children under 10 years old [The comparison of two surgery methods for treatment of supracondylar fracture in children under 10 years old in Ayatollah Kashani hospital]. en.irct.ir/trial/6916 (first received 6 November 2011).
Ducic 2016a {published data only}
-
- Ducic S, Radlovic V, Bukva B, Radojicic Z, Vrgoc G, Brkic I, et al. A prospective randomised non-blinded comparison of conventional and Dorgan's crossed pins for paediatric supracondylar humeral fractures. Injury 2016;47(11):2479-83. [PMID: ] - PubMed
Ercin 2016 {published data only}
-
- Ercin E, Bilgili MG, Baca E, Basaran SH, Bayrak A, Kural C, et al. Medial mini-open versus percutaneous pin fixation for type III supracondylar fractures in children. Turkish Journal of Trauma and Emergency Surgery 2016;22(4):350-4. [PMID: ] - PubMed
Foead 2004 {published data only}
-
- Foead A, Penafort R, Saw A, Sengupta S. Comparison of two methods of percutaneous pin fixation in displaced supracondylar fractures of the humerus in children. Journal of Orthopaedic Surgery (Hong Kong) 2004;12(1):76-82. [PMID: ] - PubMed
Gaston 2010 {published and unpublished data}
-
- Gaston RG, Cates TB, Blanco JC. Crossed versus lateral-entry pin fixation of type 3 supracondylar fractures in children. In: American Academy of Orthopaedic Surgeons Annual Meeting; 2007 Feb 14-18; San Diego (CA). 2007.
-
- Gaston RG, Cates TB, Devito D, Schmitz M, Schrader T, Busch M, et al. Medial and lateral pin versus lateral-entry pin fixation for type 3 supracondylar fractures in children: a prospective, surgeon-randomized study. Journal of Pediatric Orthopaedics 2010;30(8):799-806. [PMID: ] - PubMed
-
- Marson BA. [personal communication]. Email to: G Gaston 26 November 2020.
Gholap 2020 {published data only}
-
- Gholap A, Wokhlu A, Gholap P. Gartlands type III supracondylar humerus fractures - cross k-wiring versus lateral k-wiring: a preliminary study. International Journal of Orthopaedics Sciences 2020;6(1):1259-62.
Gopinathan 2018 {published and unpublished data}
-
- Marson BA. [personal communication]. Email to: P Behera 18 September 2020.
Jain 2019 {published data only}
-
- Jain S, Agrawal S, Banshiwal RC. Comparative study of posterior intrafocal with lateral pinning versus cross pinning for extension type supracondylar fracture humerus in children. National Journal of Clinical Orthopaedics 2019;3(1):134-9.
Kaewpornsawan 2001 {published data only}
-
- Kaewpornsawan K. Comparison between closed reduction with percutaneous pinning and open reduction with pinning in children with closed totally displaced supracondylar humeral fractures: a randomized controlled trial. Journal of Pediatric Orthopaedics. Part B 2001;10(2):131-7. [PMID: ] - PubMed
Kalia 2018 {published data only}
-
- Kalia G, Singh N. Prospective randomised comparison study of 60 cases of type 2 and type 3 supracondylar fractures of humerus in children using conventional cross K wire fixation vs Dorgan's lateral fixation. Indian Journal of Applied Research 2018;8(7):70-1.
Kocher 2007 {published data only}
-
- Kocher MS, Kasser JR, Waters PM, Bae D, Snyder BD, Hresko MT, et al. Lateral entry compared with medial and lateral entry pin fixation for completely displaced supracondylar humeral fractures in children: a randomized clinical trial. Journal of Bone and Joint Surgery - Series A 2007;89(4):706-12. [PMID: ] - PubMed
-
- Mininder SK, Waters PM, Kasser JR, Hresko MT, Bae DS, Hedequist DJ, et al. Lateral vs medial/lateral pinning of type 3 supracondylar humerus fractures in children: an RCT. In: American Academy of Orthopaedic Surgeons Annual Meeting; 2006 Mar 22-26; Chicago (IL). 2006.
-
- Yen YM, Kocher MS. Lateral entry compared with medial and lateral entry pin fixation for completely displaced supracondylar humeral fractures in children. Journal of Bone and Joint Surgery - Series A 2008;90(Suppl 2 (part 1)):20-30. [PMID: ] - PubMed
Kumar 2021 {published data only}
-
- Kumar M, Singh JP. Comparative evaluation of result of conservative versus percuteneous K-wire fixation in type III supracondylar fracture humerus in children. International Journal of Health and Clinical Research 2021;4(5):145-8.
Kuzma 2014 {published and unpublished data}
-
- ACTRN12610000026022. Randomized clinical trial to compare straight arm skin traction and olecranon skeletal traction for displaced supracondylar fractures of the humerus in children [Randomised clinical trial to compare the effect of straight arm skin traction versus olecranon skeletal traction on cubitus varus deformity and range of movement in children with displaced supracondylar fracture of the humerus]. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=320763&isRe... (first received 11 January 2010).
-
- Kuzma J. A comparison of skin vs. skeletal traction in the management of childhood humeral supracondylar fractures: randomized clinical trial. Internet Journal of Orthopedic Surgery 2014;22(1):1-7.
Maity 2012 {published data only}
-
- Maity A, Saha D, Roy D. A prospective randomised, controlled clinical trial comparing medial and lateral entry pinning with lateral entry pinning for percutaneous fixation of displaced extension type supracondylar fractures of the humerus in children. Journal of Orthopaedic Surgery and Research 2012;7:6-14. [PMID: ] - PMC - PubMed
Majeed 2020 {published data only}
-
- Majeed F, Saddique M, Nasir H, Shams A. Comparison of closed reduction and percutaneous cross verses parallel k wire fixation in supracondylar fractures of the humerus in children. Professional Medical Journal 2020;27(03):476-80.
Mandal 2018 {published data only}
-
- Mandal J, Sarkar P, Singh A, Banka PK, Bindumadhavan S. Study of clinical and radiological outcomes in paediatric supracondylar humerus fractures treated with 3 lateral pins versus crossed pins. International Journal of Orthopaedics Sciences 2018;4(2):745-9.
Mulpuri 2016 {published data only}
-
- Mulpuri K, Dobbe A, Schaeffer E, Miyanji F, Alvarez C, Cooper A, et al. Management of displaced supracondylar fractures of the humerus using lateral versus cross k wires: a prospective randomised trial. In: Pediatric Orthopaedic Society of North America (POSNA) Annual Meeting; 2016 Apr 27-30; Indianapolis (IN). 2016:e-Poster #8.
-
- Mulpuri K, Dobbe A, Schaeffer E, Miyanji F, Alvarez C, Cooper A, et al. Management of displaced supracondylar fractures of the humerus using lateral versus cross k wires: a prospective randomised trial. Orthopaedic Proceedings. The British Editorial Society of Bone & Joint Surgery 2016;98-B(Suppl 21):93.
-
- NCT00358787. Management of displaced supracondylar fractures of the humerus using lateral vs. crossed K-wires [Management of displaced supracondylar fractures of the humerus using lateral versus cross K wires: a prospective randomized clinical trial]. clinicaltrials.gov/ct2/show/record/NCT00358787 (first received 1 August 2006).
Naik 2017 {published and unpublished data}
-
- Marson BA. [personal communication]. Email to: GM Sharma 29 September 2020.
Naveen 2017 {published data only}
-
- Naveen PR, Chaitanya PR. A prospective study of crossed versus lateral only pinning in the treatment of displaced supracondylar fractures of the humerus in children. International Journal of Orthopaedics Sciences 2017;3(3):400-4.
Oakley 2009 {published and unpublished data}
-
- ACTRN12607000047493. A randomised controlled trial of two methods of immobilising supracondylar fractures of the humerus [Is immobilisation with collar and cuff or backslab and sling associated with less pain and better parent satisfaction in children with minimally displaced supracondylar fractures of the humerus?]. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=81800&isRev... (first received 12 January 2007).
-
- Marson BA. [personal communication]. Email to: E Oakley 13 November 2020.
-
- Oakley E, Barnett P, Babl FE. Backslab versus nonbackslab for immobilization of undisplaced supracondylar fractures: a randomized trial. Pediatric Emergency Care 2009;25(7):452-6. [PMID: ] - PubMed
Othman 2017 {published data only}
-
- Othman M, Nahla A, El-Malt A. A comparative study of three percutaneous pinning techniques for paediatric supracondylar humeral fractures. ARC Journal of Othopedics 2017;2(2):11-9.
Palange 2019 {published data only}
-
- Palange ND, Prasannakumar GS, Mane A, Pawar E. A comparison between percutaneous cross k wire and lateral k wires fixation in management of Type III Gartland paediatric supracondylar fractures. International Journal of Orthopaedics Sciences 2019;5(2):119-22.
Pandey 2008 {published data only}
-
- Pandey S, Shrestha D, Gorg M, Singh GK, Singh MP. Treatment of supracondylar fracture of the humerus (type IIB and III) in children: a prospective randomized controlled trial comparing two methods. Kathmandu University Medical Journal 2008;6(23):310-8. - PubMed
Patil 2017 {published data only}
-
- Patil SP, Gaonkar N, Pandey P, Kumar S, Shah R, Garud A, et al. A comparative study of two percutaneous pinning techniques (Cross K wire vs Lateral K wire) for Gartland type III pediatric supracondylar fracture of the humerus. International Journal of Orthopaedics Sciences 2017;3(4):665-8.
Pavone 2016 {published data only}
-
- Pavone V, Riccioli M, Testa G, Lucenti L, De Cristo C, Condorelli G, et al. Surgical treatment of displaced supracondylar pediatric humerus fractures: comparison of two pinning techniques. Journal of Functional Morphology and Kinesiology 2016;1(1):39-47.
Prashant 2016 {published data only}
-
- Prashant K, Lakhotia D, Bhattacharyya TD, Mahanta AK, Ravoof A. A comparative study of two percutaneous pinning techniques (lateral vs medial-lateral) for Gartland type III pediatric supracondylar fracture of the humerus. Journal of Orthopaedics and Traumatology 2016;17(3):223-9. [PMID: ] - PMC - PubMed
Raj 2018 {unpublished data only}
-
- Raj KN. Comparision of Functional Outcome Between Traditional and Lateral Crossed Pinning in Supra condylar Humerus Fractures of Children [Masters thesis]. Chennai: Madras Medical College, 2018.
Rakha 2020 {published data only}
-
- Rahka A, Khan RD, Arshad A, Khan ZAli, Ahmad S, Mahmood S. Comparison of efficacy between open and close reduction in supracondylar fracture of humerus in children using Flynn’s criteria. Annals of Punjab Medical College (APMC) 2020;14(1):32-6.
Ray 2019 {published data only}
-
- Ray B, Waikhom S. A comparative study of closed reduction and percutaneous crossed pinning vs open reduction and crossed pinning in Gartland Type III supracondylar fracture of humerus in children. International Journal of Scientific Research 2019;8(3):15-9.
Rizk 2019 {published data only}
-
- Rizk AS, Kandil MI. Conventional versus lateral cross-pinning (Dorgan’s technique) for fixation of displaced pediatric supracondylar humeral fractures: a randomized comparative study. Egyptian Orthopaedic Journal 2019;53:348-58.
Sadek 2018 {published data only}
-
- Sadek AA, Ibrahim MI, Elazab HE, Abdel Rahman HH. Comparison of fixation of supracondylar humeral fractures in children by lateral cross-wiring technique versus traditional lateral pinning. Sohag Medical Journal 2018;22(1):265-71.
Saeed 2020 {published data only}
-
- Saeed UB, Waseem M, Hassan AR, Khan ZA, Gill D, Ahmad S. Supracondylar fracture, buried vs non buried K wires. Professional Medical Journal 2020;27(03):467-71.
Said 2015 {unpublished data only}
-
- Said EA. Crossed-pin configuration versus lateral pins in treatment of supracondylar humeral fracture in children. In: 36th Société Internationale de Chirurgie Orthopédique et de Traumatologie'(SICOT) Orthopaedic World Congress; 2015 Sep 17-19; Guangzhou (China). 2015.
Sankar 2019 {published data only}
-
- Sankar S, D’Souza JJ, Debuka E, Vyas T, Jagani N. The functional outcome of displaced supracondylar fracture humerus in children treated by open reduction and internal fixation by lateral pins compared to medial and lateral pins: a prospective study. National Journal of Clinical Orthopaedics 2019;3(2):78-84.
Shafi‐Ur‐Rehman 2013 {published data only}
-
- Shafi-Ur-Rehman, Hayat K, Bajwa A, Yousaf M, Rehman A, Shafaq SA. To compare the outcome of patients with supracondylar fractures of humerus treated by cross K-wires and lateral entry K-wires in children. Pakistan Journal of Medical and Health Sciences 2013;7(2):500-5.
-
- Shah ZA, Arif U. Displaced supracondylar humeral fractures; treatment among children: crossed versus lateral pinning. Professional Medical Journal 2013;20(5):818-24.
Shah 2017 {published data only}
-
- Shah SA, Asimuddin M. Management of supracondylar fractures of the humerus in children: conservative versus operative. International Journal of Orthopaedics 2017;3(1):14-20.
-
- Shah SA, Asimuddin M. Management of supracondylar fractures of the humerus in children: conservative versus operative. Scholars Journal of Applied Medical Sciences 2016;4(6B):1960-9.
Shamma 2020 {published data only}
-
- Shamma AE, Moawad Abd El-Motalb M, Abd El-Hamed ME, Tash E. Lateral divergent pinning versus lateral parallel pinning in management of supracondylar fractures of the humerus in children. Al-Azhar Medical Journal 2020;49(2):513-24.
Subash 2020 {published data only}
-
- Subash Y, Natarajan S, Lydia M. A study comparing two different pinning techniques in supracondylar fractures of the humerus. International Journal of Research in Pharmaceutical Sciences 2020;11(Special Issue 2):48-53.
Tripuraneni 2009 {published data only}
-
- Tripuraneni KR, Bosch PP, Schwend RM, Yaste JJ. Prospective, surgeon-randomized evaluation of crossed pins versus lateral pins for unstable supracondylar humerus fractures in children. Journal of Pediatric Orthopaedics. Part B 2009;18(2):93-8. [PMID: ] - PubMed
Vaidya 2009 {published data only}
-
- Vaidya SM. Percutaneous fixation of displaced supracondylar fracture in children comparing lateral with medial and lateral pin [Masters thesis]. Mahé, Seychelles: University of Seychelles, 2009.
Zhu 2016 {published data only}
-
- Zhu YL, Hu W, Yu XB, Wu YS, Sun LJ. A comparative study of two closed reduction methods for pediatric supracondylar humeral fractures. Journal of Orthopaedic Science 2016;21(5):609-13. [PMID: ] - PubMed
References to studies excluded from this review
AboHasan 2020 {published data only}
-
- AboHasan MA, Idrees K, Fahmy MH. Closed reduction and lateral percutaneous pin fixation for displaced supracondylar humerus fractures in children. Zagazig University Medical Journal 2020;26(2):233-8.
Aktekin 2008 {published data only}
-
- Aktekin CN, Toprak A, Ozturk AM, Altay M, Ozkurt B, Tabak AY. Open reduction via posterior triceps sparing approach in comparison with closed treatment of posteromedial displaced Gartland type III supracondylar humerus fractures. Journal of Pediatric Orthopaedics. Part B 2008;17(4):171-8. - PubMed
Arif 2014 {published data only}
-
- Arif M, Azeem M, Khurshid J. Surgical outcome of medial and lateral approach in treatment of paediatriac humeral supracondylar fracture. Journal of Sheikh Zayed Medical College 2014;5(3):644-7.
Arif 2017 {published data only}
-
- Arif M, Akram R, Zaman AU, Ahmad I, Aziz A. Outcome of lateral approach for displaced supracondylar humerus fractures in children. Pakistan Journal of Medical and Health Sciences 2017;11(3):825-8.
Ariyawatkul 2016 {published data only}
-
- Ariyawatkul T, Eamsobhana P, Kaewpornsawan K. The necessity of fixation in Gartland type 2 supracondylar fracture of the distal humerus in children (modified Gartland type 2A and 2B). Journal of Pediatric Orthopaedics. Part B 2016;25(2):159-64. - PubMed
Arnala 1991 {published data only}
-
- Arnala I, Paananen H, Lindell-Iwan L. Supracondylar fractures of the humerus in children. European Journal of Pediatric Surgery 1991;1(1):27-9. - PubMed
Balanescu 2013 {published data only}
-
- Balanescu R, Ulici A, Rosca D, Topor L, Barbu M. Neurovascular abnormalities in Gartland III supracondylar fractures in children. Chirurgia (Bucuresti) 2013;108(2):241-4. - PubMed
Bales 2010 {published data only}
-
- Bales JG, Spencer HT, Wong MA, Fong YJ, Zionts LE, Silva M. The effects of surgical delay on the outcome of pediatric supracondylar humeral fractures. Journal of Pediatric Orthopedics 2010;30(8):785-91. - PubMed
Bulbul 2011 {published data only}
-
- Bulbul M, Ayanoglu S, Imren Y, Kahraman S, Esenyel CZ, Gurbuz H. Does two parallel lateral-only pin configuration provide stable osteosynthesis for pediatric supracondylar humerus fractures? Nobel Medicus 2011;7(3):36-40.
Chen 2001 {published data only}
-
- Chen RS, Liu XS, Lin XM, Feng M, Zhu JM, Ye FQ. Supracondylar extension fracture of the humerus in children. Journal of Bone and Joint Surgery. British Volume 2001;83-B(6):883-7. - PubMed
Diri 2003 {published data only}
-
- Diri B, Tomak Y, Karaismailoglu TN. The treatment of displaced supracondylar fractures of the humerus in children (an evaluation of three different treatment methods). Turkish Journal of Trauma & Emergency Surgery 2003;9(1):62-9. - PubMed
Ducic 2016b {published data only}
-
- Ducic S, Bumbasirevic M, Radlovic V, Nikic P, Bukumiric Z, Brdar R, et al. Displaced supracondylar humeral fractures in children: comparison of three treatment approaches. Srpski Arhiv Za Celokupno Lekarstvo 2016;144(1-2):46-51. - PubMed
El‐Ngehy 2018 {published data only}
-
- El-Ngehy Alaa AM, Eladawy Amr M, El-Sharkawi Walid F, Naeem Muhammed MG. Crossed pinning versus two lateral wires in the management of displaced supracondylar humerus fractures in children. Zagazig University Medical Journal 2018;24(6):467-72.
Ensafdaran 2005 {published data only}
-
- Ensafdaran A, Emami MJ, Borghei M. A comparative study of lateral approach versus posterior approach for the surgical treatment of supracondylar fractures of the humerus in children. Medical Journal of The Islamic Republic of Iran (MJIRI) 2005;19(3):213-7.
Eren 2005 {published data only}
-
- Eren A, Ozkut AT, Altintas F, Guven M. Comparison between the lateral and medial approaches in terms of functional and cosmetic results in the surgical treatment of type III supracondylar humeral fractures in children. Acta Orthopaedica et Traumatologica Turcica 2005;39(3):199-204. - PubMed
Fahmy 2009 {published data only}
-
- Fahmy MA, Hatata MZ, Al-Seesi H. Posterior intrafocal pinning for extension-type supracondylar fractures of the humerus in children. Journal of Bone and Joint Surgery - Series B 2009;91(9):1232-6. - PubMed
Hegazy 2020 {published data only}
-
- Hegazy MO, Meselhy MA, EL-Nabasy AA. Lateral divergent pinning versus lateral parallel pinning in management of supracondylar fractures of the humerus in children. Benha Journal of Applied Sciences 2020;5(6 (part 2)):1-6.
Keskin 2014 {published data only}
-
- Keskin D, Sen H. The comparative evaluation of treatment outcomes in pediatric displaced supracondylar humerus fractures managed with either open or closed reduction and percutaneous pinning. Acta Chirurgiae Orthopaedicae et Traumatologiae Cechoslovaca 2014;81(6):380-6. - PubMed
Khan 2007 {published data only}
-
- Khan AQ, Goel S, Abbas M, Sherwani MK. Percutaneous K-wiring for Gartland type III supracondylar humerus fractures in children. Saudi Medical Journal 2007;28(4):603-6. - PubMed
Lee 2008 {published data only}
-
- Lee YH, Lee SK, Kim BS, Chung MS, Baek GH, Gong HS, et al. Three lateral divergent or parallel pin fixations for the treatment of displaced supracondylar humerus fractures in children. Journal of Pediatric Orthopaedics 2008;28(4):417-22. - PubMed
Li 2013 {published data only}
-
- Li WQ, Guo YM, He J, Lu S. Dynamic external fixation for stabilizing Baumman angle during midanaphase in supracondylar fracture of humerus in children. China Journal of Orthopaedics and Traumatology 2013;26(8):656-8. - PubMed
Li 2017 {published data only}
-
- Li J, Fu D, Yu C, Wang S, Ze R, Tang X. Surgical management of delayed irreducible Gartland III supracondylar fractures in children: open reduction and internal fixation versus external fixation. Journal of Shoulder and Elbow Surgery 2017;26(2):299-304. - PubMed
Marashi 2013 {published data only}
NCT00904137 {published data only}
-
- NCT00904137. Treatment of type I supracondylar fractures of the humerus. clinicaltrials.gov/ct2/show/NCT00904137 (first received 19 May 2009).
Pescatori 2012 {published data only}
-
- Pescatori E, Memeo A, Brivio A, Trapletti A, Camurri S, Pedretti L, et al. Supracondylar humerus fractures in children: a comparison of experiences. Journal of Pediatric Orthopaedics. Part B 2012;21(6):505-13. - PubMed
Rawoot 2014 {unpublished data only}
-
- Rawoot A, du Toit J, Ikram A. The treatment of Gartland 2 and 3 supracondylar humerus fractures in children in either a prone or supine position: practical implications for future treatment. British Editorial Society of Bone & Joint Surgery 2014;96:11.
Roy 2019 {published data only}
-
- Roy MK, Alam MT, Rahman MW, Islam MS, Sayeed KA, Kamal MZ, et al. Comparative study of stabilization of humerus supracondylar fracture in children by percutaneous pinning from lateral side and both sides. Mymensingh Medical Journal: MMJ 2019;28(1):15-22. - PubMed
Sadik 2015 {published data only}
-
- Sadik Diaa G. Medial and lateral percutaneous fixation versus lateral fixation for treatment of Gartland type ii, iii supracondylar fracture of humerus in children. Iraqi Journal of Medical Sciences 2015;13(2):183-90.
Shah 2013 {published data only}
-
- Shah ZA, Arif U. Displaced supracondylar humeral fractures; treatment among children: crossed versus lateral pinning. Professional Medical Journal 2013;20(5):818-24.
Shoaib 2003 {published data only}
-
- Shoaib M, Hussain A, Kamran H, Ali J. Outcome of closed reduction and casting in displaced supracondylar fracture of humerus in children. Journal of Ayub Medical College, Abbottabad : JAMC 2003;15(4):23-5. - PubMed
Siddiq 2020 {published data only}
-
- Siddiq K, ullah Mehmood A, Hameed MH, Chishti MK, Ali MN, Hussain N. Comparison of outcome with medial versus lateral approach for operative fixation of superacondylar humeral fractures in paediatric patients. Professional Medical Journal 2020;27(10):2045-9.
Silva 2018 {published data only}
-
- Silva M, Sadlik G, Avoian T, Ebramzadeh E. A removable long-arm soft cast to treat nondisplaced pediatric elbow fractures: a randomized, controlled trial. Journal of Pediatric Orthopaedics 2018;38(4):223-9. - PubMed
Sutton 1992 {published data only}
-
- Sutton WR, Greene WB, Georgopoulos G, Dameron TB Jr. Displaced supracondylar humeral fractures in children. A comparison of results and costs in patients treated by skeletal traction versus percutaneous pinning. Clinical Orthopaedics & Related Research 1992;278:81-7. - PubMed
Venkatadass 2015 {published data only}
-
- Venkatadass K, Balachandar G, Rajasekaran S. Is prone position Ideal for manipulation and pinning of displaced pediatric extension-type supracondylar fractures of humerus? A randomized control trial. Journal of Pediatric Orthopedics 2015;35(7):672-6. - PubMed
Young 2012 {published data only}
-
- Young S, Fevang JM, Gullaksen G, Nilsen PT, Engesaeter LB. Parent and patient satisfaction after treatment for supracondylar humerus fractures in 139 children: no difference between skeletal traction and crossed pin fixation at long-term followup. Advances in Orthopaedics 2012;2012:[6 p.]. - PMC - PubMed
References to studies awaiting assessment
Afridi 2002 {published data only}
-
- Afridi HD, Ansar AH. Prospective randomised study of the management of supracondylar (humerus) fractures in children. Medical Channel Journal 2002;8(1):41-3.
Andreasi 1985 {published data only}
-
- Andreasi A. Comparison of two methods of percutaneous osteosynthesis with Kirschner wires in diastatic supracondylar fractures of the humerus in children. Minerva Ortopedica 1985;36(5):295-300.
Bing 2017 {published data only}
-
- Bing C, Zhenglin L, Yanjun G. Clinical observation of early closed reduction and flexible lateral Kirschner wire external fixation for supracondylar fracture of humerus in children. Journal of Mathematical Medicine 2017;30:1288–90.
Boparai 2006 {published data only}
-
- Boparai RS, Diwan D. Supracondylar fractures in children - closed reduction vs open reduction. Indian Journal of Orthopaedics 2006;40(2):103-7.
Botchu 2006 {published data only}
-
- Botchu R, Shetty S, Shetty V, Shetty AC. Displaced supracondylar fractures of humerus in children - to pin or not to? European Journal of Trauma 2006;32(Suppl 1):162.
Evans 1998 {published data only}
-
- Evans SC, Hamilton P, Godette G, Torode IP, Dickens DR, Broughton NS, et al. Supracondylar fractures of the humerus in children: a randomised clinical trial [abstract]. Journal of Bone and Joint Surgery: British Volume 1998;80(Suppl 2):140-1.
He 2009 {published data only}
-
- He BX, Zhang B, Tan YJ. Comparison of clinical effects of various external fixation for the treatment of humeral supracondylar fracture. China Journal of Orthopaedics and Traumatology 2009;22(3):190-2. - PubMed
Lu 2011 {published data only}
-
- Lu X, Luo B, Li K. Different methods for treatment of patients with supracondylar fractures of the humerus: a randomized study. China Modern Medicine 2011;18:74–5.
NCT04582123 {published data only}
-
- NCT04582123. Comparison of cross pin configurations in supracondylar humerus fracture treatment: 2 pins versus 3 pins. clinicaltrials.gov/show/NCT04582123 (first received 9 October 2020).
Sapkota 2019 {published data only}
-
- Sapkota K, Wahegaonkar K, Ranjeet N, Thapa U, Onta P. Comparison of cross pinning versus lateral three pins in type three supracondylar fracture of distal humerus in children. Asian Journal of Medical Sciences 2019;10:58-61.
References to ongoing studies
ACTRN12612000480886 {published data only}
-
- ACTRN12612000480886. Study of treatment methods for undisplaced supracondylar humeral (elbow) fractures in children [The effect of three different types of external immobilisation methods comparing pain during application and functional outcome for children with undisplaced supracondylar humeral fractures]. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=362446&isRe... (first received 2 June 2012).
CTRI/2020/06/025504 {published data only}
-
- CTRI/2020/06/025504. Comparison of short term functional and radiological outcomes between two versus three lateral pin fixation techniques in fractures of lower part on arm bone in children [Comparison of short term functional and radiological outcomes between two versus three lateral pinning techniques in Gartland type III supracondylar humerus fractures in children - a randomized control trial]. www.who.int/trialsearch/Trial2.aspx?TrialID=CTRI/2020/06/025504 (first received 1 June 2020).
PACTR201702001960109 {published data only}
-
- PACTR201702001960109. Treatment of supracondylar humerus fractures in children [Comparison between crossing wires versus two lateral wires in the management of displaced supracondylar humerus in children]. trialsearch.who.int/?TrialID=PACTR201702001960109 (first received 3 January 2017).
Additional references
American Academy of Orthopaedic Surgeons 2011
-
- American Academy of Orthopaedic Surgeons. AAOS Guideline of the treatment of pediatric supracondylar humerus fractures; September 2011. www.aaos.org/research/guidelines/SupracondylarFracture/Summary_of_Recs.pdf (accessed 5 August 2019).
Arnould 2004
-
- Arnould C, Penta M, Renders A, Thonnard J-L. ABILHAND-Kids: a measure of manual ability in children with cerebral palsy. Neurology 2004;63(6):1045-52. - PubMed
Babal 2010
-
- Babal JC, Mehlman CT, Klein G. Nerve injuries associated with pediatric supracondylar humeral fractures: a meta-analysis. Journal of Pediatric Orthopaedics 2010;30(3):253-63. - PubMed
Barr 2014
Beaton 2005
-
- Beaton DE, Wright JG, Katz JN, The Upper Extremity Collaborative Group. Development of the QuickDASH: comparison of three item-reduction approaches. Journal of Bone and Joint Surgery 2005;87A(5):1038-46. - PubMed
Bieri 1990
-
- Bieri D, Reeve RA, Champion GD, Addicoat L, Ziegler JB. The Faces Pain Scale for the self-assessment of the severity of pain experienced by children: development, initial validation, and preliminary investigation for ratio scale properties. Pain 1990;41(2):139-50. - PubMed
Brauer 2007
-
- Brauer CA, Lee BM, Bae DS, Waters PM, Kocher MS. A systematic review of medial and lateral entry pinning versus lateral entry pinning for supracondylar fractures of the humerus. Journal of Pediatric Orthopaedics 2007;27(2):181-6. - PubMed
British Orthopaedic Association 2014
-
- British Orthopaedic Association, British Society for Children's Orthopaedic Surgery. Supracondylar Fractures of the Humerus in Children. London (UK): British Orthopaedic Association, 2014.
Carrazzone 2021
-
- Carrazzone OL, Barbachan Mansur NS, Matsunaga FT, Matsumoto MH, Faloppa F, Belloti JC, et al. Crossed versus lateral K-wire fixation of supracondylar fractures of the humerus in children: a meta-analysis of randomized controlled trials. Journal of Shoulder and Elbow Surgery 2021;30(2):439-48. - PubMed
Catena 2019
-
- Catena N, Calevo MG, Fracassetti D, Moharamzadeh D, Origo C, De Pellegrin M. Risk of ulnar nerve injury during cross-pinning in supine and prone position for supracondylar humeral fractures in children: a recent literature review. European Journal of Orthopaedic Surgery & Traumatology 2019;29(6):1169-75. - PubMed
Chapleau 2011
Cheng 1999
-
- Cheng JC, Ng BK, Ying SY, Lam PK. A 10-year study of the changes in the pattern and treatment of 6,493 fractures. Journal of Pediatric Orthopedics 1999;19(3):344-50. - PubMed
Daltroy 1998
-
- Daltroy LH, Liang MH, Fossel AH, Goldberg MJ. The POSNA pediatric musculoskeletal functional health questionnaire: report on reliability, validity, and sensitivity to change. Pediatric Outcomes Instrument Development Group. Pediatric Orthopaedic Society of North America. Journal of Pediatric Orthopedics 1998;18(5):561-71. - PubMed
Dekker 2016
-
- Dekker AE, Krijnen P, Schipper IB. Results of crossed versus lateral entry K-wire fixation of displaced pediatric supracondylar humeral fractures: a systematic review and meta-analysis. Injury 2016;47(11):2391-8. - PubMed
Delniotis 2019
-
- Delniotis I, Delniotis A, Saloupis P, Gavriilidou A, Galanis N, Kyriakou A, et al. Management of the pediatric pulseless supracondylar humeral fracture: a systematic review and comparison study of "Watchful Expectancy Strategy" versus Surgical Exploration of the Brachial Artery. Annals of Vascular Surgery 2019;55:260-71. - PubMed
Del Valle‐Hernández 2017
-
- Del Valle-Hernández E, Marrero-Barrera PA, Beaton D, Bravo D, Santiago S, Guzmán-Pérez H, et al. Complications associated with pediatric supracondylar humeral fractures. Puerto Rico Health Sciences Journal 2017;36(1):37-40. - PubMed
De Pellegrin 2018
-
- De Pellegrin M, Fracassetti D, Moharamzadeh D, Origo C, Catena N. Advantages and disadvantages of the prone position in the surgical treatment of supracondylar humerus fractures in children. A literature review. Injury 2018;49 Suppl 3:S37-42. - PubMed
Egger 1997
Farnsworth 1998
-
- Farnsworth CL, Silva PD, Mubarak SJ. Etiology of supracondylar humerus fractures. Journal of Pediatric Orthopedics 1998;18(1):38-42. - PubMed
Farrow 2018
-
- Farrow L, Ablett AD, Mills L, Barker S. Early versus delayed surgery for paediatric supracondylar humeral fractures in the absence of vascular compromise: a systematic review and meta-analysis. Bone & Joint Journal 2018;100-b(12):1535-41. - PubMed
Flynn 1974
-
- Flynn JC, Matthews JG, Benoit RL. Blind pinning of displaced supracondylar fractures of the humerus in children. Sixteen years' experience with long-term follow-up. Journal of Bone and Joint Surgery 1974;56(2):263-72. - PubMed
Gartland 1959
-
- Gartland JJ. Management of supracondylar fractures of the humerus in children. Surgery, Gynecology & Obstetrics 1959;109(2):145-54. - PubMed
Golden 2007
-
- Golden DW, Jhee JT, Gilpin SP, Sawyer JR. Elbow range of motion and clinical carrying angle in a healthy pediatric population. Journal of Pediatric Orthopaedics B 2007;16(2):144-9. - PubMed
Griffin 2008
-
- Griffin KJ, Walsh SR, Tang TY, Boyle JR, Hayes PD. The pink pulseless hand: a review of the literature regarding management of vascular complications of supracondylar humeral fractures in children. European Journal of Vascular and Endovascular Surgery 2008;36(6):697-702. - PubMed
Hell 2021
Higgins 2011
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from training.cochrane.org/handbook/archive/v5.1/.
Holt 2017
-
- Holt JB, Glass NA, Bedard NA, Weinstein SL, Shah AS. Emerging U.S. national trends in the treatment of pediatric supracondylar humeral fractures. Journal of Bone and Joint Surgery 2017;99(8):681-7. - PubMed
Holt 2018
-
- Holt JB, Glass NA, Shah AS. Understanding the epidemiology of pediatric supracondylar humeral fractures in the United States. Journal of Pediatric Orthopedics 2018;38(5):e245-51. - PubMed
Horst 2011
-
- Horst M, Altermatt S, Weber DM, Weil R, Ramseier LE. Pitfalls of lateral external fixation for supracondylar humeral fractures in children. European Journal of Trauma and Emergency Surgery 2011;37(4):405-10. - PubMed
Houshian 2011
-
- Houshian S, Mehdi B, Larsen MS. The epidemiology of elbow fracture in children: analysis of 355 fractures, with special reference to supracondylar humerus fractures. Journal of Orthopaedic Science 2001;6(4):312-15. - PubMed
Hudak 1996
-
- Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: the DASH (Disabilities of the Arm, Shoulder and Hand) [Corrected]. The Upper Extremity Collaborative Group (UECG). American Journal of Industrial Medicine 1996;29(6):602-8. - PubMed
Kurer 1990
-
- Kurer MH, Regan MW. Completely displaced supracondylar fracture of the humerus in children: a review of 1708 comparable cases. Clinical Orthopaedics and Related Research 1990;256:205-14. - PubMed
Lefebvre 2019
-
- Lefebvre C, Glanville J, Briscoe S, Littlewood A, Marshall C, Metzendorf MI, et al. Chapter 4: Searching for and selecting studies. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.0 (updated July 2019). Cochrane, 2019. Available from: www.training.cochrane.org/handbook.
Leitch 2006
-
- Leitch KK, Kay RM, Femino JD, Tolo VT, Storer SK, Skaggs DL. Treatment of multidirectionally unstable supracondylar humeral fractures in children: a modified Gartland type-IV fracture. Journal of Bone and Joint Surgery 2006;88(5):980-5. - PubMed
Lin‐Guo 2018
Loizou 2009
-
- Loizou CL, Simillis C, Hutchinson JR. A systematic review of early versus delayed treatment for type III supracondylar humeral fractures in children. Injury 2009;40(3):245-8. - PubMed
Mangat 2009
-
- Mangat KS, Martin AG, Bache CE. The ‘pulseless pink’ hand after supracondylar fracture of the humerus in children. Journal of Bone and Joint Surgery. British Volume 2009;91-B(11):1521-5. - PubMed
Marson 2020a
-
- Marson BA, Craxford S, Deshmukh SR, Grindlay DJ, Manning JC, Ollivere BJ. Quality of patient-reported outcomes used for quality of life, physical function, and functional capacity in trials of childhood fractures. Bone and Joint Journal 2020;102-B(12):1599–1607. - PubMed
Marson 2020c
Morrey 1993
-
- Morrey BF. Functional evaluation of the elbow. In: Morrey BF, editors(s). The Elbow and Its Disorders. Philadelphia (PA): Saunders, 1993:86.
Na 2018
NICE 2016
-
- National Institute for Health and Care Excellent (NICE). Fractures (non-complex): assessment and management. NICE guideline [NG38]; February 2016. www.nice.org.uk/guidance/ng38/chapter/recommendations (accessed 11 February 2021).
O'Connor 2016
Omid 2008
-
- Omid R, Choi PD, Skaggs DL. Supracondylar humeral fractures in children. Journal of Bone and Joint Surgery. American Volume 2008;90(5):1121-32. - PubMed
Patriota 2017
Pretell 2010
Pretell‐Mazzini 2010a
Pretell‐Mazzini 2010b
Review Manager 2014 [Computer program]
-
- Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Saylor 1999
-
- Saylor CF, Swenson CC, Reynolds SS, Taylor M. The Pediatric Emotional Distress Scale: a brief screening measure for young children exposed to traumatic events. Journal of Clinical Child Psychology 1999;28(1):70-1. - PubMed
Schünemann 2019
-
- Schünemann HJ, Higgins JP, Vist GE, Glasziou P, Akl EA, Skoetz N, et al. Chapter 14: Completing ‘Summary of findings’ tables and grading the certainty of the evidence. Draft version (29 January 2019) for inclusion in: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al (editors). Cochrane Handbook for Systematic Reviews of Interventions, Version 6.1 (updated September 2020), Cochrane, 2020. Available from handbook.cochrane.org.
Sharma 2013
-
- Sharma K, Mansur DI, Khanal K, Haque MK. Variation of carrying angle with age, sex, height and special reference to side. Kathmandu University Medical Journal (KUMJ) 2013;11(44):315-8. - PubMed
Sinikumpu 2016
-
- Sinikumpu JJ, Victorzon S, Pokka T, Lindholm EL, Peljo T, Serlo W. The long-term outcome of childhood supracondylar humeral fractures: a population-based follow up study with a minimum follow up of ten years and normal matched comparisons. Bone & Joint Journal 2016;98-B(10):1410-7. - PubMed
Slobogean 2010
-
- Slobogean BL, Jackman H, Tennant S, Slobogean GP, Mulpuri K. Iatrogenic ulnar nerve injury after the surgical treatment of displaced supracondylar fractures of the humerus: number needed to harm, a systematic review. Journal of Children's Orthopaedics 2010;30(5):430-6. - PubMed
Slongo 2006
-
- Slongo T, Audigé L, Schlickewei W, Clavert JM, Hunter J. Development and validation of the AO pediatric comprehensive classification of long bone fractures by the Pediatric Expert Group of the AO Foundation in collaboration with AO Clinical Investigation and Documentation and the International Association for Pediatric Traumatology. Journal of Pediatric Orthopedics 2006;26(1):43-9. - PubMed
Terpstra 2022
Tzatzairis 2021
-
- Tzatzairis T, Firth G, Loke WJ, Serlis A, Ramachandran M. Does compliance with BOAST guidelines matter for displaced supracondylar fractures in children?: the experience of a tertiary referral major trauma centre over a 3.5-year period. Journal of Pediatric Orthopaedics. Part B 2021;1(30):154-60. - PubMed
Vaquero‐Picado 2018
White 2010
-
- White L, Mehlman CT, Crawford AH. Perfused, pulseless, and puzzling: a systematic review of vascular injuries in pediatric supracondylar humerus fractures and results of a POSNA questionnaire. Journal of Pediatric Orthopaedics 2010;30(4):328-35. - PubMed
Wilkins 1996
-
- Wilkins KE. Fractures and dislocations of the elbow region. In: Rookwood CA Jr, Wilkins KE, King RE, editors(s). Fractures in Children. 4th edition. Vol. 3. Philadelphia (PA): Lippincott-Raven, 1996.
Wille 2010
Woratanarat 2012
-
- Woratanarat P, Angsanuntsukh C, Rattanasiri S, Attia J, Woratanarat T, Thakkinstian A. Meta-analysis of pinning in supracondylar fracture of the humerus in children. Journal of Orthopaedic Trauma 2012;26(1):48-53. - PubMed
Yeomans 2018
-
- Yeomans D, Graham SM, Mkandawire NC, Harrison WJ, Perry DC. Conservative management of displaced paediatric supracondylar fractures: a systematic review. Tropical Doctor 2018;48(4):359-65. - PubMed
Young 2000
-
- Young NL, Williams JI, Yoshida KK, Wright JG. Measurement properties of the activities scale for kids. Journal of Clinical Epidemiology 2000;52(2):125-37. - PubMed
Yousri 2012
-
- Yousri T, Tarassoli P, Whitehouse M, Monsell F, Khan WS. Systematic review of randomized controlled trials comparing efficacy of crossed versus lateral K-wire fixation in extension type Gartland type III supracondylar fractures of the humerus in children. Ortopedia, Traumatologia, Rehabilitacja 2012;14(5):397-405. - PubMed
References to other published versions of this review
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous