

Right colectomy from open to robotic - a single-center experience with functional outcomes in a learning-curve setting
- PMID: 35678902
- PMCID: PMC9640414
- DOI: 10.1007/s00423-022-02576-8
Right colectomy from open to robotic - a single-center experience with functional outcomes in a learning-curve setting
Abstract
Purpose: Right colectomy (RC) is a frequently performed procedure. Beneath standard conventional open surgery (COS), various minimally invasive techniques had been introduced. Several advantages had recently been described for robotic approaches over COS or conventional laparoscopy. Nevertheless, novel minimally invasive techniques require continuous benchmarking against standard COS to gain maximum patient safety. Bowel dysfunction is a frequent problem after RC. Together with general complication rates postoperative bowel recovery are used as surrogate parameters for postoperative patient outcome in this study.
Methods: Retrospective, 10-year single-center analysis of consecutive patients who underwent sequentially either COS (n = 22), robotic-assisted (ECA: n = 39), or total robotic surgery (ICA: n = 56) for oncologic RC was performed.
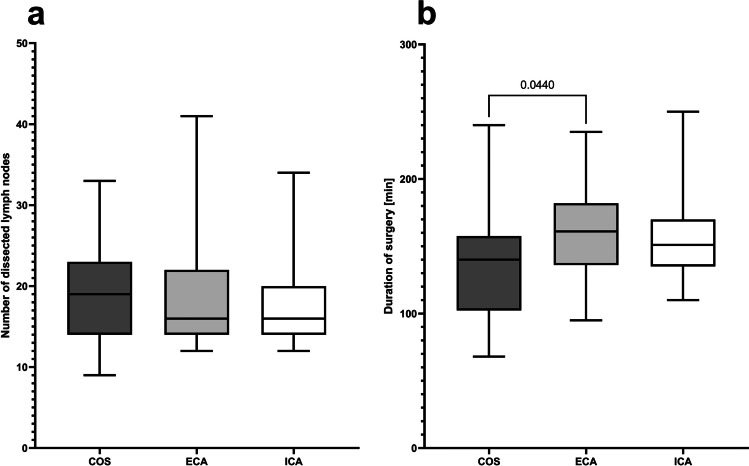
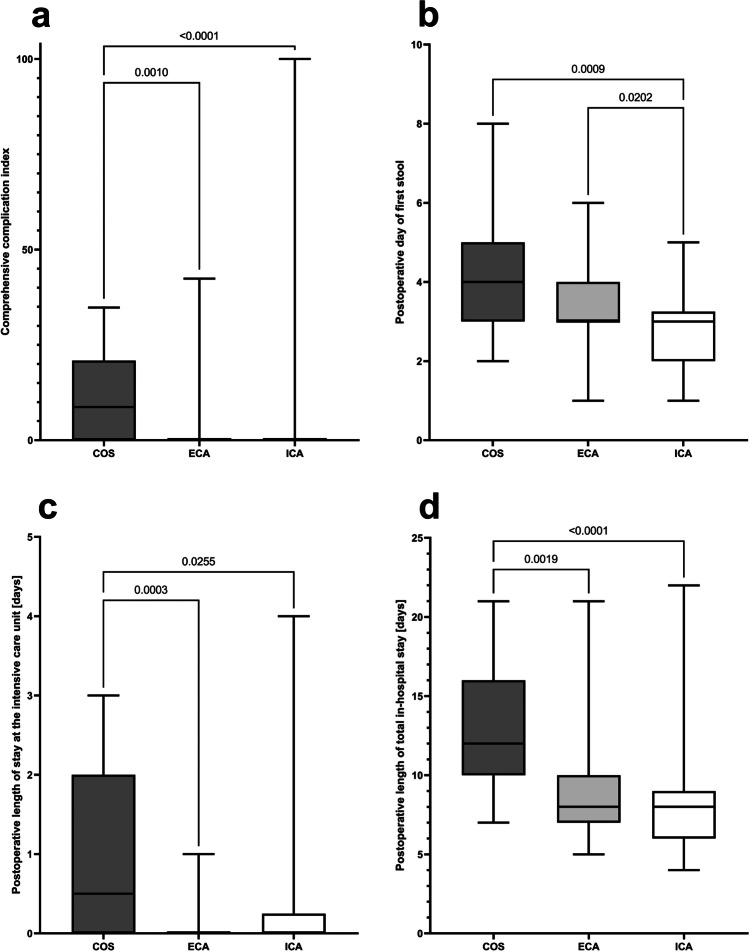
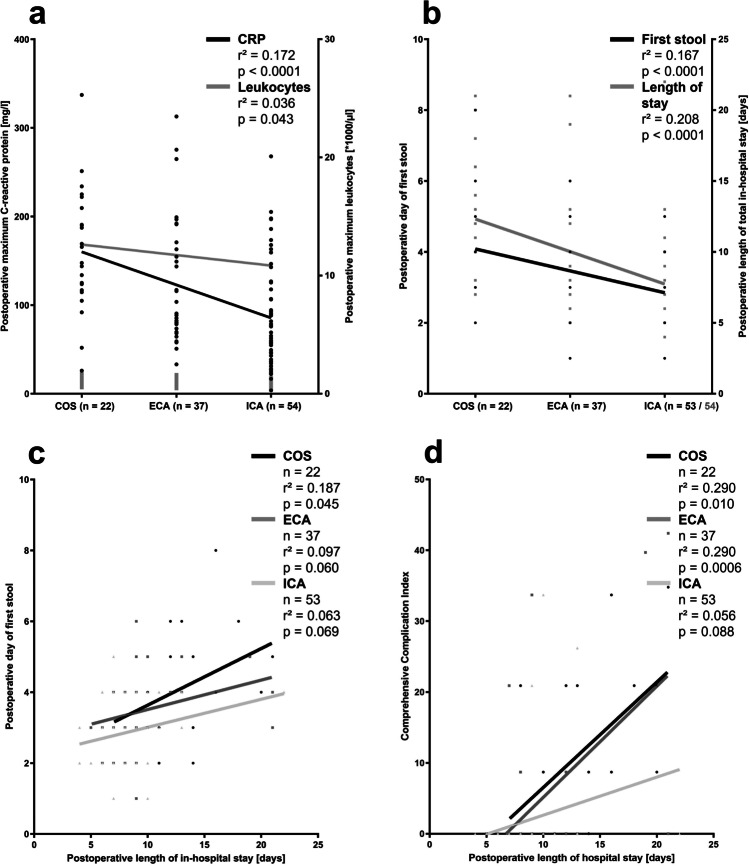
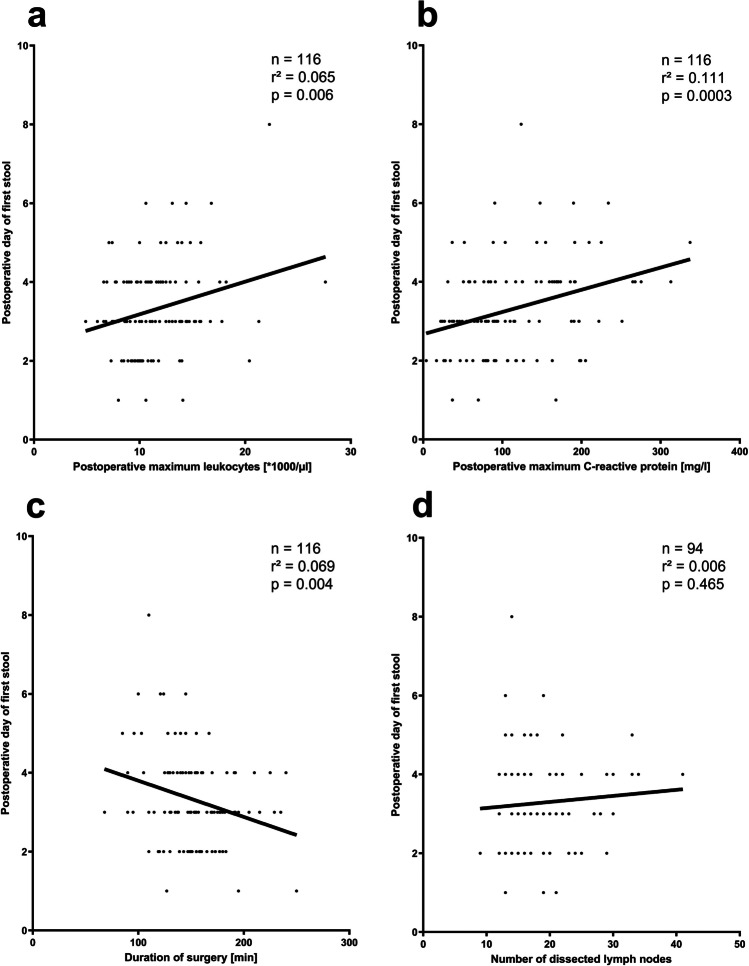
Results: The conversion from robotic to open surgery rate was low (overall: 3.2%). Slightly longer duration of surgery had been observed during the early phase after introduction of the robotic program to RC (ECA versus COS, p = 0.044), but not anymore thereafter (versus ICA). No differences were observed in oncologic parameters including rates of tumor-negative margins, lymph node-positive patients, and lymph node yield during mesocolic excision. Both robotic approaches are beneficial regarding postoperative complication rates, especially wound infections, and shorter length of in-hospital stay compared with COS. The duration until first postoperative stool is the shortest after ICA (COS: 4 [2-8] days, ECA: 3 [1-6] days, ICA: 3 [1-5] days, p = 0.0004). Regression analyses reveal neither a longer duration of surgery nor the extent of mesocolic excision, but the degree of minimally invasiveness and postoperative systemic inflammation contribute to postoperative bowel dysfunction, which prolongs postoperative in-hospital stay significantly.
Conclusion: The current study reflects the institutional learning curve of oncologic RC during implementation of robotic surgery from robotic-assisted to total robotic approach without compromises in oncologic results and patient safety. However, the total robotic approach is beneficial regarding postoperative bowel recovery and general patient outcome.
Keywords: Bowel dysfunction; Complete mesocolic excision; Ileus; Intracorporal anastomosis; Right colectomy; Robot.
© 2022. The Author(s).
Conflict of interest statement
Dr. Hirschburger reports personal fees from Proctor for Intuitive surgical, personal fees from lectures for Intuitive surgical, both outside the submitted work.
Rolf Schneider reports non-financial support from Intuitive surgical, outside the submitted work.
Andreas Hecker received honoraria from KCI and MSD, independently from the content of this work.
Sophie Kraenzlein, Winfried Padberg, and Martin Reichert have nothing to declare.
Figures

References
-
- Hamilton AER, Chatfield MD, Johnson CS, Stevenson ARL. Totally robotic right hemicolectomy: a multicentre case-matched technical and peri-operative comparison of port placements and da Vinci models. J Robot Surg. 2020;14:479–491. - PubMed
-
- Juvik AF, Nielsen S, Tolstrup M-B, Lykke J, Klein M (2020) Anastomotic technique is not associated with leakage rate after right hemicolectomy. Dan. Med. J. 67: - PubMed
-
- Fleshman J, Sargent DJ, Green E, Anvari M, Stryker SJ, Beart RWJ, Hellinger M, Flanagan RJ, Peters W, Nelson H. Laparoscopic colectomy for cancer is not inferior to open surgery based on 5-year data from the COST Study Group trial. Ann Surg. 2007;246:654–655. - PubMed
-
- Buunen M, Veldkamp R, Hop WCJ, et al. Survival after laparoscopic surgery versus open surgery for colon cancer: long-term outcome of a randomised clinical trial. Lancet Oncol. 2009;10:44–52. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
