

Differential antibody production by symptomatology in SARS-CoV-2 convalescent individuals
- PMID: 35679259
- PMCID: PMC9182712
- DOI: 10.1371/journal.pone.0264298
Differential antibody production by symptomatology in SARS-CoV-2 convalescent individuals
Abstract
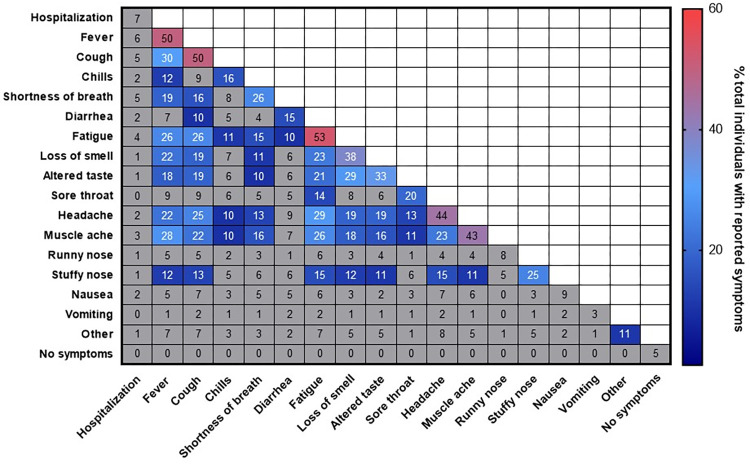
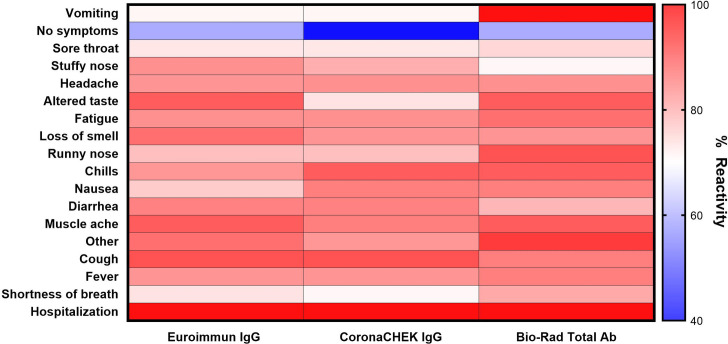
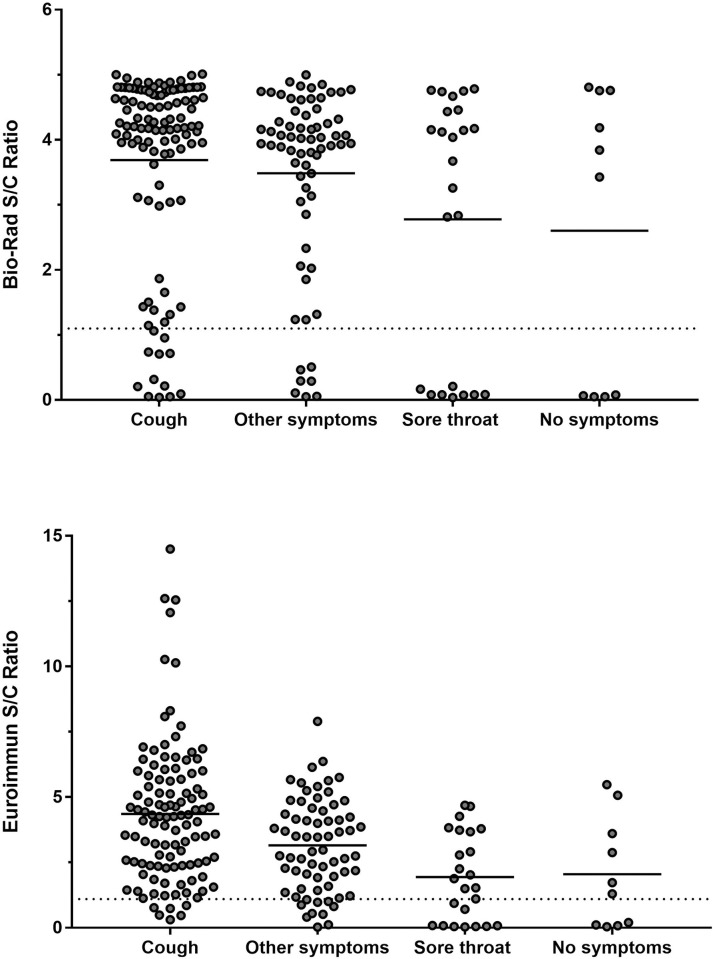
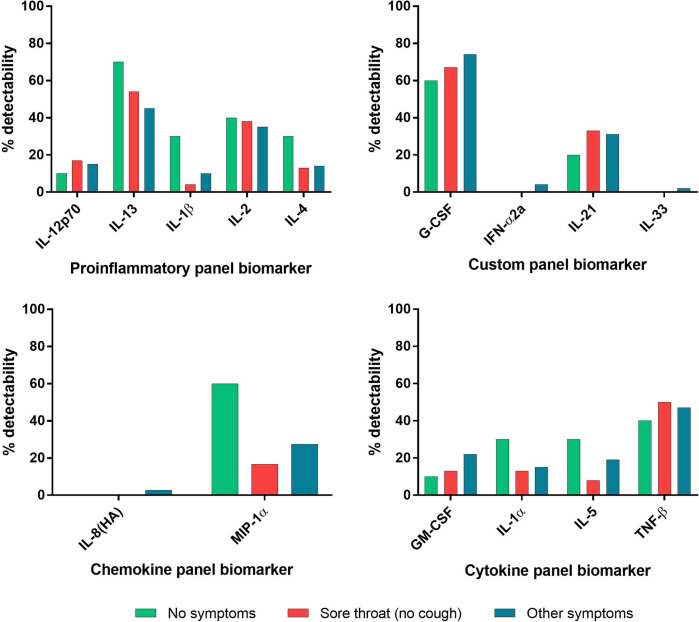
The association between COVID-19 symptoms and antibody responses against SARS-CoV-2 is poorly characterized. We analyzed antibody levels in individuals with known SARS-CoV-2 infection to identify potential antibody-symptom associations. Convalescent plasma from 216 SARS-CoV-2 RNA+ individuals with symptomatology information were tested for the presence of IgG to the spike S1 subunit (Euroimmun ELISA), IgG to receptor binding domain (RBD, CoronaCHEK rapid test), and for IgG, IgA, and IgM to nucleocapsid (N, Bio-Rad ELISA). Logistic regression was used to estimate the odds of having a COVID-19 symptom from the antibody response, adjusting for sex and age. Cough strongly associated with antibodies against S1 (adjusted odds ratio [aOR] = 5.33; 95% CI from 1.51 to 18.86) and RBD (aOR = 4.36; CI 1.49, 12.78). In contrast, sore throat significantly associated with the absence of antibodies to S1 and N (aOR = 0.25; CI 0.08, 0.80 and aOR = 0.31; 0.11, 0.91). Similarly, lack of symptoms associated with the absence of antibodies to N and RBD (aOR = 0.16; CI 0.03, 0.97 and aOR = 0.16; CI 0.03, 1.01). Cough appeared to be correlated with a seropositive result, suggesting that SARS-CoV-2 infected individuals exhibiting lower respiratory symptoms generate a robust antibody response. Conversely, those without symptoms or limited to a sore throat while infected with SARS-CoV-2 were likely to lack a detectable antibody response. These findings strongly support the notion that severity of infection correlates with robust antibody response.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Update of
-
Differential antibody production by symptomatology in SARS-CoV-2 convalescent individuals.medRxiv [Preprint]. 2022 Feb 9:2022.02.09.22270718. doi: 10.1101/2022.02.09.22270718. medRxiv. 2022. Update in: PLoS One. 2022 Jun 9;17(6):e0264298. doi: 10.1371/journal.pone.0264298. PMID: 35169815 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
